US Pharm.
2007;1:82-87.
In 2005, an estimated 20.8
million people in the United States had diabetes mellitus.1
Diabetes comprises a group of metabolic disorders resulting from a defect in
insulin production, action, or both. It is characterized by chronic
hyperglycemia and disturbances of carbohydrate, protein, and fat metabolism
that can result in microvascular, macrovascular, and neuropathic complications.
2 Type 1 diabetes results from an autoimmune destruction of the
pancreatic beta cells. This type usually is found in children and adolescents,
although the disease onset can occur at any age. Patients with type 1 diabetes
have little or no pancreatic function, a tendency to develop ketoacidosis, and
a dependency on exogenous insulin to sustain life. Type 2 diabetes is
characterized by variable degrees of insulin resistance, impaired insulin
secretion, and increased glucose production. This type is typically recognized
in adulthood but is becoming more prevalent among obese children. Furthermore,
the prevalence of type 2 diabetes increases with age. In the U.S., type 2
diabetes is more common in women than in men. The incidence also varies among
different racial and ethnic populations, with the highest incidence observed
in Native Americans, Hispanic-Americans, Asian-Americans, African-Americans,
and Pacific Islanders.3 Ninety percent of the total diagnosed cases
of diabetes are type 2, while 10% are type 1.
Monitoring
Monitoring is a
critical part of diabetes management. Patients must be well educated about the
importance of monitoring and appropriate techniques. There is an established
relationship between monitoring, therapy compliance, and risk of complications.
4 Laboratory values that are commonly monitored include glucose and
glycosylated hemoglobin (GHb) measurements.
Though generally inexpensive
and mildly invasive, glucose monitoring may be performed many times per day by
the patient in the comfort of his or her own home. Generally, patients are
instructed to monitor before and after meals. Blood samples as small as 1 mcL
may be taken from a number of sites including the finger, forearm, arm,
abdomen, thigh, and calf.5 Glucose levels can be altered by diet,
exercise, and medications.6
Evaluated every two to three
months, GHb values are directly proportional to glucose concentration and
duration of exposure.7 Although there are several species of
glycohemoglobin, HbA1c is the most prevalent and is traditionally monitored in
clinical practice.7 Usually performed in the doctor's office, this
method also requires only a small amount of blood. Achieving the optimal goal
for HbA1c (? 7%) is associated with a reduced risk of secondary
complications. Several studies have illustrated that improved glycemic control
reduces the risk of secondary complications by 35%.7 Every
percentage point decrease in HbA1c results in a significant reduction in the
risk of microvascular complications and diabetes-related deaths.4
The American Diabetes Association recommends twice-yearly monitoring in
patients with controlled glycemic levels, with more frequent evaluations in
those who have not met their glycemic goals. African-American patients tend to
have higher HbA1c values.
Monitoring Devices
With the
availability of more than 20 brands, glucose monitoring is easily achieved
with a glucose meter (usually handheld) that requires a single drop of blood.
More than 20 brands of glucose meters are available. Most differ only by the
amount of time or blood necessary to achieve a reading and memory or by the
number of test strips the machines are able to hold. Newer glucose monitors go
beyond conventional handheld devices and take samples throughout the day
without the patient's assistance. Some examples include glucose meter watches
and implanted transmitters.
Glycohemoglobin monitoring is
challenging because of the varying combinations of hemoglobins. Some
laboratories choose to report total glycosylated hemoglobin, while others
report HbA1c. Several efforts have been taken by the National Glycohemoglobin
Standardization Program (NGSP) to standardize the measurement.
The A1CNow+
With an
increase in the prevalence of diabetes and the potential serious complications
of the disease, home testing of HbA1c should be an integral part of diabetes
management. Metrika's A1CNow+ (see Figure 1) is the
first nonprescription device that patients with diabetes can use at home to
obtain immediate HbA1c results between office visits. The A1CNow+
is a portable, easy-to-use device that provides rapid HbA1c results with
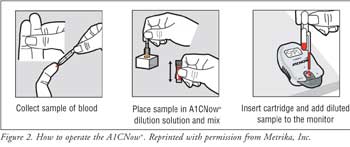
precision and accuracy.8 A1CNow+ requires approximately
10 mcL of blood. The blood is diluted with 0.69 mL of the buffered detergent
solution ferricyanide and is directly applied to the sample port. Results are
displayed in numeric form on the monitor's liquid crystal display after five
minutes. The device self-activates upon insertion of the test cartridge, and
no fasting is required before obtaining the blood sample. Test results are
expressed as %A1c, representing glucose control over the last three months.
9 Patient instructions are located in Figure 2.

Efficacy
Metrika's A1cNow
+ has undergone various studies to determine its efficacy and accuracy.
When compared to a variety of laboratory tests certified by the College of
American Pathologists, %A1c results were similar. The A1CNow+'s
results have been shown to be within 0.9% of the A1c value allowed by the NGSP.
10 In 2005, a study comparing BioRad Variant II, A1CNow+, and
a NGSP Certified laboratory test revealed that A1CNow+ was within
1% of the A1c value allowed by NGSP.11
Conclusion
Metrika's A1CNow
+ is an excellent addition to at-home testing for patients with
diabetes. Since it measures HbA1c, it allows both the patient and the
clinician to monitor overall patient progress. This device is patient-friendly
and does not require a prescription. It should supplement patient self-care
between physician visits and is not intended to replace daily monitoring.
References
1. Centers for Disease Control and Prevention Web site. Available at: www.cdc.gov/diabetes/pubs/pdf/ndfs_2005.pdf. Accessed October 31, 2006.
2. DiPiro J, Talbert R, et al. Pharmacotherapy: A Pathophysiologic Approach. 5th ed. New York: McGraw Hill; 2002:1335-1358.
3. Fauci A, Braunwald E, et al. Harrison's Principles of Internal Medicine. 16th ed. New York: McGraw-Hill; 2005:2152-2180.
4. Krapek K, King K, et al. Medication adherence and associated hemoglobin A1c in type 2 diabetes. Ann Pharmacother. 2004;38:1357-1362.
5. Dufaitre-Patouraux L, Djemli K, Vague P. How and when to use an alternative site in self-monitoring of blood glucose. Diabetes Metab. 2004;30:471-477.
6. Chin M, Cook S, et al. Barriers to providing diabetes care in community health centers. Diabetes Care. 2001;24(2):268-274.
7. Krishnamurti U, Steffes M. Glycohemoglobin: a primary predictor of the development or reversal of complications of diabetes mellitus. Clin Chem.2001;47(7):1157-1165.
8. Metrika Web site. Available at: www.metrika.com. Accessed November 2, 2006.
9. Metrika's A1CNow+ Professional-Use Product Insert. Available at: www.metrika.com. Accessed November 2, 2006.
10. Metrika comparative A1C results across laboratories. Metrika, Inc. December 2002.
11. Field study using A1cNow InView.
Metrika, Inc. December 2005.
To comment on this article, contact
editor@uspharmacist.com.



