US Pharm. 2008;33(5)(Student suppl):6-9.
Infectious mononucleosis (IM) was
first described in 1889 as glandular fever, a clinical illness characterized
by fever, fatigue, abdominal discomfort, hepatosplenomegaly (enlargement of
both the liver and spleen), and lymphadenopathy. Later observations linking
the appearance of atypical lymphocytosis helped to establish IM as a clinical
entity.1 It was not until 1968 that IM was linked to the
Epstein-Barr virus (EBV).2 EBV is one of the most ubiquitous human
herpes viruses, and it is associated with more than 90% of cases of IM.1
Epidemiology
In the United
States, more than 90% of adults between the ages of 35 and 40 test positive
for EBV and carry the virus in a latent state for life.2,3
Epidemiologic studies have shown that in nonindustrialized countries primary
infections occur earlier in life, while in developed countries seroconversion
occurs more frequently during adolescence.1,4 When primary
infection occurs during childhood, it often remains asymptomatic and
undetected.1,4 Clinical symptoms are present in 35% to 50% of cases
affecting adolescents and young adults.3
IM affects 45 in every 100,000
people, with peak incidence typically occurring between the ages of 15 and 25
years.1 Incidence in the college student population has been rated
around 15%.5 No gender differences or seasonal prevalence has been
observed.1
EBV infects and replicates
primarily in the B lymphocytes and epithelial cells of the oropharynx and
confers a lifelong latent infection.4 EBV is often found in the
saliva of infected persons and spreads to susceptible individuals by close
contact such as kissing. Therefore, IM became known as the "kissing disease."
1,3 EBV has limited viability outside the body and its spread by contact
with contaminated personal objects or eating utensils is not clear. The
Centers for Disease Control and Prevention does not recommend any special
precautions since the virus can be found even in the saliva of healthy
individuals.2,5 Reports of transmission through blood transfusions
can also be found.5 Although not conclusive, data suggest that EBV
can be transmitted through sexual intercourse, and having an increased number
of sexual partners poses a significant risk factor to seroconversion.4,6
Incubation period for IM is usually between 30 and 50 days.6
Clinical Presentation
Infectious
mononucleosis is characterized by fever, pharyngitis, splenomegaly, and
generalized lymphadenopathy (Table 1). Often the full clinical syndrome
is preceded by three to five days of prodromal symptoms consisting of
headaches, fatigue, and myalgias.5 ever usually ranges between
39.4°C and 40.6°C and can last for one to two weeks.7
Sore throat has been reported to be present in more than 85% of patients.8
Enlarged tonsils with exudate are commonly found. These clinical findings can
easily be mistaken for group A streptococci pharyngitis.7

Lymphadenopathy occurs in more
than 90% of patients with IM and affects mostly the anterior and posterior
cervical lymph nodes.6,7 The lymph nodes are symmetrical and only
moderately tender on palpation.2 Lymphadenopathy gradually resolves
within two to three weeks.7,8
Lymphocytic infiltration of
the spleen leads to splenomegaly in as many as 50% to 63% of patients with IM.
Massive spleen enlargement and spleen rupture are rare but severe
complications of IM.5-7 Hepatomegaly is present in only about 10%
of patients, and mild-to-moderate elevation of hepatic transaminases and
bilirubin can also be found.1,5,7
Skin manifestations like rash
have been reported in 3% to 19% of cases of IM.7 Rash can be
macular, papular, erythematous, or morbilliform and typically affect the trunk
and arms.1,7 The concurrent administration of the antibiotics
ampicillin and amoxicillin has been implicated in the occurrence of a
pruritic, maculopapular rash in 90% to 100% of patients.1,7 It can
persist for up to one week and does not represent hypersensitivity to these
drugs.1,7
Confirmation of the diagnosis
can be aided by laboratory examination (Table 1). The white blood cell
count often varies between 10,000 and 20,000 cells/mm3 with a
predominance of lymphocytes and monocytes up to 60% to 70%.1,6
Atypical lymphocytes are characteristic of IM. These cells are usually larger
with a lower nuclear-to-cytoplasm ratio than the mature circulating
lymphocytes.1,6 Although very common in IM, atypical lymphocytes
can also be found in other viral infections such as cytomegalovirus,
toxoplasmosis, rubella, and hepatitis, among others.1,6 Platelet
count can also be decreased but rarely drops below 50,000/mm3, and
purpura is rare.6
Heterophile antibodies are
present in 90% of IM cases and are both very sensitive and specific for the
disease. These antibodies were first described by Paul and Bunnell and are IgM
immunoglobulins that agglutinate sheep and horse red blood cells. These
antibodies can be demonstrated in high titers during the first month of the
illness and gradually decrease over the following four to six months.1,3,7
Heterophile antibodies are the
basis for a commercial test kit known as the "monospot test." The specificity
of the monospot test is very high, approaching 90%. However, sensitivity is
variable with a high false-negative rate in children less than 10 years old
and during the first week of the onset of illness.2,3 The monospot
test can detect heterophile antibodies in 70% to 90% of adolescents and adults
and is useful to confirm clinical diagnosis.2 In patients with a
negative monospot test but with clinical symptoms indicative of IM, other
heterophile-negative mononucleosis-like illness should be ruled out. The most
common causes of heterophile-negative mononucleosis-like syndrome are
cytomegalovirus, viral hepatitis, acute toxoplasmosis, group A beta-hemolytic
streptococci, and HIV-1 infections.1,2 Other serologic tests that
detect antibodies against EBV's capsid (IgM VCA) can aid final diagnosis in
selected cases.1,2
Treatment
IM is a
self-limited disease, and spontaneous recovery occurs in more than 95% of
cases. Supportive care with symptom relief, rest, and good hydration is the
mainstay of therapy.1,7
Analgesics and antipyretics
such as acetaminophen and nonsteroidal anti-inflammatory agents are
recommended for fever and pain relief. Saline gargles may be useful to
alleviate sore throat.1
Systemic corticosteroids have
been used to treat IM, but their efficacy is controversial. While some studies
have demonstrated quicker resolution of fever and sore throat, others have
failed to show any significant improvement in symptoms.1,7 A recent
Cochrane Database review evaluated the results of seven trials that
investigated the use of corticosteroids for symptom relief in IM. The review
showed a great heterogeneity among studies regarding subject inclusion
criteria, treatment protocols, and outcomes. The authors concluded that there
is a lack of evidence to recommend the use of corticosteroids in the treatment
of uncomplicated IM.9 There are also concerns of possible adverse
effects of corticosteroids in otherwise uncomplicated cases. Although
scientific data supporting the use of corticosteroids are lacking, current
indications still include IM complicated by severe airway edema, hemolytic
anemia, and thrombocytopenia.10,11
Several trials have
investigated the use of anti viral agents in the treatment of
mononucleosis. A trial of 94 patients randomly assigned to receive either oral
acyclovir and prednisolone or placebo for a total of 10 days failed to show
any significant effects on the duration of clinical symptoms.12
Significant decrease in oropharyngeal EBV shedding was demonstrated in the
same study and corroborated by others.12-14 A meta-analysis of five
randomized controlled trials that included 339 patients treated with acyclovir
showed no clinical benefit of acyclovir when compared to placebo. Inhibition
of viral shedding at the end of therapy was shown, but the effect was lost
three weeks after withdrawal of therapy. The authors concluded that there are
no clinical data to support the use of acyclovir for the treatment of IM.
15 Most symptoms associated with EBV infection result from the vigorous
body immune response against EBV, and that might explain the lack of efficacy
of antiviral agents that work by inhibiting viral replication during the lytic
phase of the infection.1
Complications
The majority of
patients with IM fully recover over a period of weeks to a few months.16
Nevertheless, cases of complications have been reported widely in the
literature.
Spleen Rupture and
Restricted Activity:
Splenomegaly is a common clinical finding in IM, and spleen rupture is a rare
but potentially life-threatening complication in adolescents and young adults.
It is estimated to occur in 0.5% of cases.5,16,17 Most spleen
ruptures occur following even mild abdominal trauma and are more likely to
occur between day 4 and 21 of the illness.17 Lymphocytic
infiltration with spleen enlargement may compromise normal anatomy and
supportive structures leading to spleen fragility.17 Rest should be
enforced and physical activity restricted with avoidance of all contact sports.
5,17 Complains of abdominal pain should be taken seriously and spleen
rupture suspected. Onset of pain may be acute or insidious and usually affect
the left upper quadrant and radiate to the left shoulder. The patient may
present in shock with a falling hematocrit.1
The duration of restricted
physical activity and the decision of when to return to sports is highly
controversial and can significantly impact the quality of life of patients,
who are often highly active young adults frequently involved in competitive
athletic activities. Physical examination with splenic palpation is generally
unreliable, with one study reporting only 17% of splenomegaly being detected
upon physical examination.10 The use of imaging studies
(ultrasound, CT scanning, MRI) may be used to help document resolution of
splenomegaly; however, cost and lack of standards limit their usefulness.
17 Generally accepted practices recommend that all strenuous activity,
including weight lifting and contact sports, be avoided during the first three
weeks of illness. A gradual return to noncontact aerobic activity can be
initiated on week 4 as long as patients are asymptomatic, well hydrated, and
with no palpable spleen.5,17 For more strenuous activity, a minimum
of four weeks is recommended.17
Airway Obstruction:
One of the most common complications of IM is airway obstruction secondary to
tonsil swelling and nasopharyngeal edema. It affects approximately 5% of
patients and often leads to hospitalization.6,15 Treatment includes
supportive care with administration of IV fluids, head of bed elevation, and
use of systemic corticosteroids.6,16
Neurologic Complications:
Even though headaches are present in 50% of IM cases, more severe neurologic
complications are present in less than 1% of cases. Meningoencephalitis is
among the most severe complications and is characterized by altered level of
consciousness and possibly seizures. Other reported neurologic complications
include Guillain-Barre syndrome, optic neuritis, and transverse myelitis.
16
Hematologic
Complications:
Transient mild thrombocytopenia is present in half of cases of mononucleosis
but rarely is severe enough to cause bleeding.16 Hemolytic anemia
has been reported to occur in 0.5% to 3% of cases. Hemolysis is generally
noted during the second or third week and resolves in four to eight weeks.
1 There is some evidence that both thrombocytopenia and hemolytic anemia
are mediated by auto-antibodies. In the more severe cases, corticosteroids may
be tried to hasten recovery.1 Mild neutropenia is common, but
neutrophils below 1,000 cells/mm3 are present in 3% of cases,
lasting from a few days to two weeks.16
Fatigue:
The first two to four weeks of illness are often marked by severe fatigue.
Malaise and mild fatigue can last up to several months. There is no convincing
evidence confirming the link between EBV infection and chronic fatigue
syndrome.6,16
EBV-associated
Malignancies: More
than 90% of the adult population who are infected with EBV carry the virus for
life as latent infection of the B lymphocytes without any adverse events.
2,3 However, in immunosuppressed individuals (i.e., transplant or AIDS
patients) or in individuals with environmental and/or genetic factors, it can
rarely result in malignancy. Lymphoproliferative disease, Hodgkin's and
Burkitt's lymphoma, and nasopharyngeal carcinoma have also been associated
with EBV.1,4
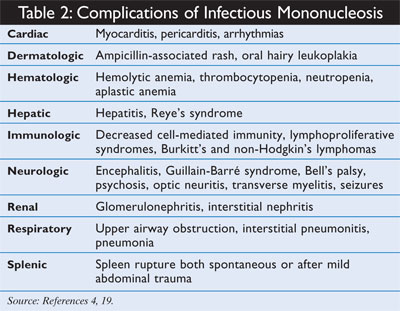
Others:
Liver enzymes are elevated two to three fold in 90% of IM cases, but jaundice
is uncommon.16,18 A list of other reported complications can be
found in Table 2.
Summary
Infectious
mononucleosis is a clinical syndrome characterized by fever, pharyngitis,
lymphadenopathy, and atypical lymphocytosis. It is caused by the Epstein-Barr
virus and primarily affects adolescents and young adults. Primary infections
acquired during childhood are usually asymptomatic. Transmission occurs by
close contact with saliva of infected individuals. Final diagnosis can be made
by a positive monospot test confirming the presence of heterophile antibodies,
although the monospot test is unreliable during the first week of illness and
in young children. Treatment consists of supportive care ensuring appropriate
hydration, rest, and use of analgesic/antipyretic agents for symptom relief.
Corticosteroids should be reserved for complicated cases with respiratory
compromise, severe thrombocytopenia, and hemolytic anemia. There is no role
for antivirals in the treatment of IM. Restricted physical activity with
avoidance of all contact sports and weight-bearing activities should be
enforced during the first three weeks after onset of symptoms to decrease the
risk of spleen rupture. Gradual return to athletic activities should be
individualized based on symptoms and clinical exam. The prognosis for IM is
good, with low incidence of complications. Acute symptoms usually resolve in
two to three weeks, but mild fatigue may persist longer.
REFERENCES
1. Johannsen EC,
Schooley RT, Kaye KM. Epstein-Barr virus (infectious mononucleosis). In:
Mandell GL, Bennett JE, Dolin R, eds. Principles and Practice of Infectious
Diseases. 6th ed. Philadelphia, PA: Churchill Livingstone; 2005:chap 135.
2. Hurt C, Tammaro D.
Diagnostic evaluation of mononucleosis-like illnesses. Am J Med.
2007;120:911-918.
3. Epstein-Barr virus
and infectious mononucleosis. National Center for Infectious Diseases. Centers
for Disease Control and Prevention. www.cdc.gov/ncidod/diseases/ebv.htm.
Accessed January 26, 2008.
4. Macsween K, Crawford
DH. Epstein-Barr virus--recent advances. Lancet Infect Dis.
2003;3:131-140.
5. Hosey RG, Rodenberg
RE. Infectious disease and the collegiate athlete. Clin Sports Med.
2007;26:449-471.
6. Rimsza ME, Kirk GM.
Common medical problems of the college student. Pediatr Clin N Am.
2005;52:9-24.
7. Katz BZ.
Epstein-Barr virus (mononucleosis and lymphoproliferative disorders). In: Long
SS, ed. Principles and Practice of Pediatric Infectious Diseases. 2nd
ed. Philadelphia, PA: Churchill Livingstone; 2003.
8. Page CL, Diehl JJ.
Upper respiratory tract infections in athletes. Clin Sports Med.
2007;26:345-359.
9. Candy B, Hotopf M.
Steroids for symptom control in infectious mononucleosis. Cochrane Database
Syst Rev. 2006;3:CD004402.
10. Ebell M.
Epstein-Barr virus infectious mononucleosis. Am Fam Physician.
2004;70:1279-1287,1289-1290.
11. Thompson SK, Doerr
TD, Hengerer AS. Infectious mononucleosis and corticosteroids. Management
practices and outcomes. Arch Otolaryngol Head Neck Surg.
2005;131:900-904.
12. Tynell E, Aurelius
E, Brandell A, et al. Acyclovir and prednisolone treatment of acute infectious
mononucleosis: a multicenter, double-blind, placebo-controlled study. J
Infect Dis.1996;174:324-331.
13. van der Horst C,
Joncas J, Ahronheim G, et al. Lack of effect of peroral acyclovir for the
treatment of acute infectious mononucleosis. J Infect Dis.
1991;164:788-792.
14. Andersson J,
Britton S, Ernberg I, et al. Effect of acyclovir on infectious mononucleosis:
a double-blind, placebo controlled study. J Infect Dis. 1986;
153:283-290.
15. Torre D, Tambini R.
Acyclovir for treatment of infectious mononucleosis: a meta-analysis. Scan
J Infect Dis. 1999;31:543-547.
16. Jenson HB. Acute
complications of Epstein-Barr virus infectious mononucleosis. Curr Opin
Pediatr. 2000;12:263-268.
17. Waninger KN, Harcke
HT. Determination of safe return to play for athletes recovering from
infectious mononucleosis. A review of the literature. Clin J Sport Med.
2005;15:410-416.
18. Roberts JR.
Infectious mononucleosis: clinical characteristics, treatment and
complications. Emerg Med News. 2001;23:20-25.
19. Straus SE, Cohen
JI, Tosato G, Meier J. Epstein-Barr virus infections: biology, pathogenesis
and management. Ann Intern Med. 1993;118:45-58.
To comment on this article,
contact rdavidson@jobson.com.


