US Pharm. 32(7):HS-18-HS-25.
Sarcoidosis is a systemic granulomatous
disease of unknown origin primarily affecting the lungs and lymphatic systems
of the body. It was first described in 1877 and has continued to fascinate
both clinicians and scientists since that time.1 Sarcoidosis
commonly affects young and middle-aged adults. The lifetime risk for
sarcoidosis in the United States is 0.85% for Caucasians and 2.4% for African
Americans. The estimated prevalence is in the range of 1 to 40 cases per
100,000, with an age-adjusted annual incidence rate in the U.S. of 35.5 per
100,000 for African Americans and 10.9 per 100,000 for whites.1-4
In recent years, an increased understanding of the pathologic and immunologic
basis of this disease has improved treatment. This article will serve as an
introduction for pharmacists to the pathology, immunology, diagnosis, clinical
presentation, and treatment of sarcoidosis, with a focus on pulmonary
sarcoidosis since the lungs are the most common site of granuloma formation.
Etiology, Pathology,
Immunology
While the etiology
of sarcoidosis is unknown, genetic, infectious, and environmental factors have
been implicated as possible causes.5 Epstein Barr, coxsackie B
virus, Propionibacterium acnes, Mycobacterium species,
aluminum, zirconium, clay, and pine tree pollen are all examples of postulated
causative factors.1 Regardless of the cause, it appears that T
helper 1 (Th1) lymphocytes play a central role in the immune
response.5 The initial response to some infectious, genetic, or
environmental antigen is a release of interleukin-2 and tumor necrosis factor
gamma (TNF-gamma) from Th1 cells, which in turn recruits more
immune cells to the area of inflammation. The net result is an amplification
loop involving antigen-recognition, proinflammatory cytokine release, cell
activation, and recruitment. These cells accumulate within the lungs and other
affected tissues, eventually leading to the formation of noncaseating
granulomas.6,7 This local immune response and granuloma formation
leads to the tissue and organ destruction characteristic of sarcoidosis. In
the lungs, about 75% of the granulomas are located close to or within the
connective tissue sheath of bronchioles and subpleural spaces. The pulmonary
vasculature is also involved in more than 50% of patients.1,8-10
Sarcoid granulomas either resolve or leave behind fibrotic changes. End-stage
sarcoidosis causes parenchymal fibrosis and honey-combing of the lung.
1,9,10
Clinical Presentation
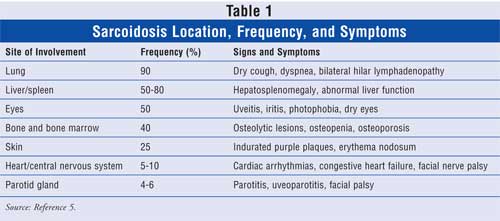
The clinical
symptoms of sarcoidosis may present in many different ways depending on the
patient's ethnicity and the chronicity, site, extent of involvement of the
organ, and the activity of the granulomas (TABLE 1).5,11
Nonspecific symptoms such as fever, fatigue, malaise, and weight loss may
occur in up to one third of sarcoidosis patients. Pulmonary sarcoidosis occurs
in more than 90% of patients.1 Other, less common forms include
cutaneous, cardiac, lymphoid, hepatic, neurologic, and musculoskeletal
sarcoidosis. Patients may have a combination of any of these forms of the
disease.
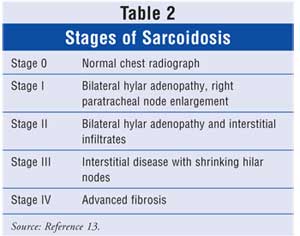
There are five radiographic stages
of pulmonary sarcoidosis, shown in TABLE 2.13 Thirty percent
to 55% of pulmonary sarcoidosis patients present with symptoms including
dyspnea, dry cough, and chest pain. Other clinical findings include decreased
forced expiratory volume, vital capacity, and diffusing capacity. Anemia,
lymphocytopenia, elevated erythrocyte sedimentation rate, increased liver
function tests, hypercalcemia, and hypercalcemic nephropathy are also common
findings.5,12
The four goals of a diagnostic workup for sarcoidosis patients are to 1) provide histologic confirmation of the disease; 2) assess the extent and severity of organ involvement; 3) assess whether the disease is stable or likely to progress; and 4) determine if therapy will be beneficial for the patient.1 Initial studies that should be performed include a history and physical exam, pulmonary function tests, complete blood count, serum chemistries, and a tuberculin skin test. 1
The diagnosis of pulmonary
sarcoidosis relies on three main findings: 1) the presence of tight,
well-formed noncaseating granulomas and a rim of lymphocytes and fibroblasts
in the outer margin of the granulomas; 2) perilymphatic interstitial
distribution of granulomas; and 3) exclusion of an alternative cause.
1,8,9,14
While spontaneous remissions occur
in nearly two thirds of patients, the course is chronic or progressive in 10%
to 30%.1,2,15-17 Fatalities have been reported in 1% to 5% of
patients, usually due to respiratory failure, central nervous system
involvement, or myocardial involvement.1,16,17
Treatment
For many patients,
systemic treatment is not necessary and the decision for systemic therapy
varies between treatment centers, with some groups treating one third of
patients and others treating more than two thirds.12,18-21
Corticosteroids continue to be the mainstay of treatment, but appropriate
usage can be unclear. The most recent consensus statement on sarcoidosis from
the American Thoracic Society, European Respiratory Society, and World
Association of Sarcoidosis and Other Granulomatous Disorders1
clearly recommends systemic therapy with corticosteroids for cardiac disease,
neurologic disease, eye disease not responding to topical therapy, and
patients with hypercalcemia. Topical steroids should be sufficient in patients
with mild disease such as skin lesions, anterior uveitis, or cough.
Most patients with symptomatic
progressive pulmonary disease will be treated with corticosteroids as well.
1,20,22,23 The recommended dose is 20 to 60 mg/day of prednisone or its
equivalent on alternate days. Patients should be reevaluated for a response
after one to three months of therapy. If the patient responds, then the dose
can be tapered to 5 to 10 mg/day or an every-other-day regimen for a minimum
of 12 months. Most patients improve and stabilize on corticosteroids, but
relapses occur in 16% to 74% of patients as the amount of drug is tapered or
discontinued.1
For those patients who do not
respond to corticosteroids or who need persistent corticosteroids,
antimalarial agents or cytotoxic agents should be considered.1,24
These medications have a theoretical benefit due to their immune-modulating
actions and have shown variable benefit in sarcoidosis patients either alone
or in a steroid-sparing combination. Methotrexate has been shown in
small-scale studies 1,25-30 to be beneficial in both new and
refractory cases. It can be used alone or with low-dose steroids. Recommended
doses are 10 to 20 mg once a week.1 Studies have shown that
azathioprine may be beneficial in chronically treated patients with or without
prednisone.31-33 The recommended dose is 50 to 200 mg per day.1
For severe refractory patients, cyclophosphamide has shown benefit at a dose
of 50 to 150 mg per day.1 Due to significant toxicity, it is now
considered a third-line agent.13 Both chloroquine and
hydroxychloroquine have shown benefit in the treatment of sarcoidosis, but due
to increased risk of retinopathy and blindness, chloroquine is the lesser
preferred agent of the two. Hydroxychloroquine is recommended at a dose of 200
to 400 mg per day.1,13,36,37 Combination therapy protocols usually
involve corticosteroids and a second-line agent with a gradual taper of the
steroid over three to six months as allowed by the patient's clinical status,
leaving the second drug as the main therapeutic agent.6
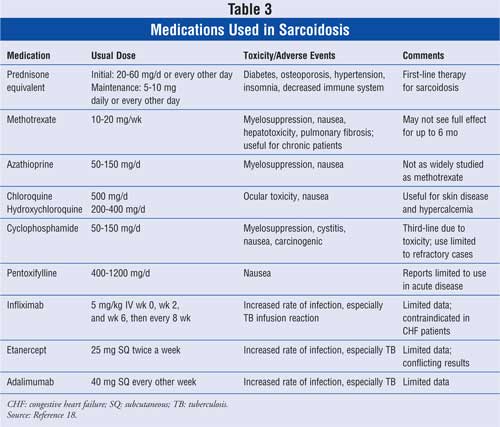
In recent years, medications
affecting TNF-alpha have been evaluated for use in sarcoidosis (TABLE 3
). Pentoxifylline, a phosphodiesterase inhibitor that inhibits the release of
TNF-alpha from alveolar macrophages, showed benefit in an open-label trial.
38 Infliximab and adalimumab, TNF-alpha inhibitors, and etanercept, a
TNF-alpha receptor blocker, have also been evaluated. These agents have shown
mixed results in small case studies and trials,39-44 but no
large-scale studies evaluating their efficacy have been performed to date.
13 Pending publication of randomized clinical trials, the use of
TNF-alpha blockade in sarcoidosis should remain in the realm of experimental
treatment.45
Conclusion
Sarcoidosis is a
disease that can affect any part of the body, but most commonly presents in
the lungs. While the exact cause of sarcoidosis still remains a mystery, the
pathologic and immunologic response of the body is becoming better understood.
The medication therapy for this debilitating disease is also not clear-cut.
Medications that have immune-modifying effects have shown benefit in
sarcoidosis in small case studies and limited controlled trials.
Corticosteroids remain first-line agents and bring about remission in many
patients. For those 10% to 30% of patients who have a chronic course of
illness, steroids are not always the best long-term option. The use of
cytotoxic agents, hydroxychloroquine, and medications affecting TNF-alpha have
been studied, but the results are mixed. Pharmacists should be well informed
of the signs and symptoms of sarcoidosis as well as its treatment. Due to the
inherent toxicity of many of these medications, patient education about side
effects and monitoring parameters of these medications are of the utmost
importance. As readily accessible health care providers, pharmacists are in a
unique position to inform patients about sarcoidosis, review the side effects
and monitor parameters of prescribed medications, and educate patients on the
most current treatment options.
References
1. Hunninghake GW,
Costabel U, et al. ATS, ERS, WASOG statement on sarcoidosis. American Thoracic
Society, European Respiratory Society, World Association of Sarcoidosis and
Other Granulomatous Disorders. Am J Respir Crit Care Med.
1999;160:736-755.
2. Henke CE, Henke G,
et al. The epidemiology of sarcoidosis in Rochester, Minnesota: a
population-based study of incidence and survival. Am J Epidemiol.
1986;123:840-845.
3. Ryhicki BA, Popovich
MJ, et al. Racial differences in sarcoidosis incidence: a 5 year study in a
health maintenance organization. Am J Epidemiol. 1999;145:234-241.
4. Bresnitz EA, Strom
BL. Epidemiology of sarcoidosis. Epidemiol Rev. 1983;5:124-156.
5. Suresh L, Radfar L.
Oral sarcoidosis: a review of literature. Oral Dis. 2005;11:138-145.
6. Barnard J, Lee SN.
Sarcoidosis: immunology, rheumatic involvement, and therapeutics. Curr Opin
Rheumatol. 2001;13:84-91.
7. Moling O, Sechi LA,
et al. Mycobacterium marinum, a further infectious agent associated with
sarcoidosis: the polyetiology hypothesis. Scand J Infect Dis.
2006;38:148-152.
8. Kitaichi M.
Pathology of pulmonary sarcoidosis. Clin Dermatol. 1986;4:108-115.
9. Rosen Y,
Sarcoidosis. In: Dail DH, Hammer SP, eds. Pulmonary Pathology. 2nd ed.
New York, NY: Springer-Verlag; 1994;13-645.
10. Colby LV.
Interstitial lung disease. In: Thurlbeck W, Churg A, eds. Pathology of the
Lung. 2nd ed. New York, NY: Thieme Medical Publishers; 1995:589-737.
11. Wilcox A, Bharadwaj
P, et al. Bone sarcoidosis. Curr Opin Rheumatol. 2000;12:321-330.
12. Rizzato G,
Montemurro L, et al. The late follow-up of chronic sarcoid patients previously
treated with corticosteroids. Sarcoidosis. 1998;15:52-58.
13. Bonfioli AA,
Fernando O. Sarcoidosis. Semin Ophthalmol. 2005;20:177-182.
14. Freiman DG, Hardy
HL. Beryllium disease: the relation of pulmonary pathology to clinical course
and prognosis based on a study of 130 cases from the U.S. beryllium case
registry. Hum Pathol. 1970;1:25-44.
15. Neville E, Walker
AN, et al. Prognostic factors predicting the outcome of sarcoidosis: an
analysis of 818 patients. Q J Med. 1983;52:525-533.
16. Romer FK.
Presentation of sarcoidosis and outcome of pulmonary changes. Dan Bull Med
. 1982;29:27-32.
17. Hillerdal G, Nou E,
et al. Sarcoidosis: epidemiology and prognosis. A 15 year European study.
Am Rev Respir Dis. 1984;130:29-32.
18. Baughman RP, Lower
EE, et al. Sarcoidosis. Lancet. 2003;361:1111-1118.
19. Gibson GJ, Prescott
RJ, et al. British thoracic society sarcoidosis study: effects of long term
corticosteroid treatment. Thorax. 1996;51:238-247.
20. Hunninghake GW,
Gilbert S, et al. Outcome of the treatment for sarcoidosis. Am J Respir
Crit Care Med. 1994;149:893-898.
21. Gottlieb JE, Israel
HL, et al. Outcome in sarcoidosis. The relationship of relapse to
corticosteroid therapy. Chest. 1997;111:623-631.
22. Semenzato G.
Assessment of disease activity in sarcoidosis: deeds and misdeeds [editorial].
Sarcoidosis. 1993;10:100-103.
23. Baughman R, Lower
E, et al. Treatment modalities for sarcoidosis. Clin Pulm Med.
1994;1:223-231.
24. Lynch JP, McCune
WJ. Immunosuppressive and cytotoxic pharmacotherapy for pulmonary disorders.
Am J Respir Crit Care Med. 1997;155:395-420.
25. Henderson CA,
Ilchyayhn A, et al. Laryngeal and cutaneous sarcoidosis treated with
methotrexate. J R Soc Med. 1994;17:632-633.
26. Isreal H. The
treatment of sarcoidosis. Postgrad Med J. 1970;46:537-540.
27. Kaye O, Palazzo E,
et al. Low-dose methotrexate: an effective corticosteroid-sparing agent in the
musculoskeletal manifestations of sarcoidosis. Br J Rheumatol.
1995;34:642-644.
28. Lacher MJ.
Spontaneous remission or response to methotrexate in sarcoidosis. Ann
Intern Med. 1968;69:1247-1248.
29. Lower EE, Baughman
RP. The use of low dose methotrexate in refractory sarcoidosis. Am J Med Sci
. 1990;299:153-157.
30. Lower EE, Baughman
RP. Prolonged use of methotrexate for sarcoidosis. Arch Intern Med.
1995;155:846-851.
31. Sharma O, Hughes D,
et al. Immunosuppressive therapy with azathioprine in sarcoidosis. In:
Levinsky L, Macholoa F, eds. Fifth International Conference on Sarcoidosis
and Other Granulomatous Disorders. Prague, Czechoslovakia: Universita
Karlova; 1971:635-637.
32. Hof D, Hof P, et
al. Long-term use of azathioprine as a steroid sparing treatment for chronic
sarcoidosis [abstract]. Am J Respir Crit Care Med. 1996;153:A870.
33. Pachcco Y, Marcchal
F, et al. Azathioprine treatment of chronic pulmonary sarcoidosis.
Sarcoidosis. 1995;2:107-113.
34. Demeter SL.
Myocardial sarcoidosis unresponsive to steroids. Treatment with
cyclophosphamide. Chest. 1988;94:202-203.
35. Zuber M, Defer G,
et al. Efficacy of cyclophosphamide in sarcoid radiculomyclitia [letter]. J
Neurol Neurosurg. 1992;55:166-167.
36. Chloroquine in the
treatment of sarcoidosis. A report from the Reseach Committee of the British
Tuberculosis Association. Tubercle. 1967;48(4):257-272.
37. Zic JA, Horowitz
DH, et al. Treatment of cutaneous sarcoidosis with chloroquine: a review of
the literature. Arch Dermatol. 1991;127:1034-1040.
38. Zabel P, Entzian P,
et al. Pentoxifylline in treatment of sarcoidosis. Am J Respir Crit Care Med
. 1997;155:1665-1669.
39. Baughman RP, Lower
EE. Infliximab for refractory sarcoidosis. Sarcoidosis Vasc Diffuse Lung Dis
. 2001;18:70-74.
40. Yee AM, Pochapin
MB. Treatment of complicated sarcoidosis with infliximab anti-tumor
necrosis-alpha therapy. Ann Intern Med. 2001;135:27-31.
41. Baughman RP,
Bradley DA, et al. Double blind randomized trial of a tumor necrosis factor
receptor antagonist (etanercept) for treatment of chronic ocular sarcoidosis.
Am J Respir Crit Care Med. 2002;165:A495.
42. Utz JP, Limper AH,
et al. Etanercept for the treatment of stage II and III progressive pulmonary
sarcoidosis. Chest. 2007;124:177-185.
43. Baughman RP, Drent
M, et al. Infliximab for the therapy of chronic sarcoidosis. Am J Respir
Crit Care Med. 2006;174:795-802.
44. Callejas-Rubio JL,
Ortego-Centeno N, et al. Treatment of therapy-resistant sarcoidosis with
adalimumab. Clin Rheumatol. 2006;25:596-597.
45. Denys BG, Bogaerts
Y, et al. Steroid-resistant sarcoidosis: is antagonism of TNF-alpha the
answer? Clin Sci. 2007;112:281-289.
To comment on this article, contact editor@uspharmacist.com.



