US Pharm.
2008;33(8):28-30.
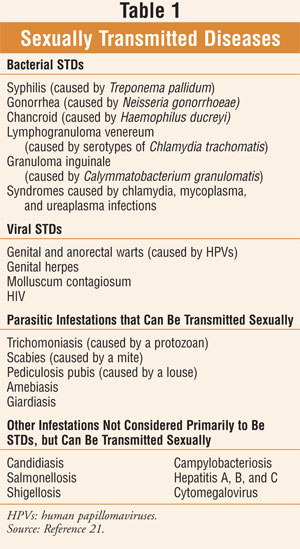
Sexually
transmitted diseases (STDs) (TABLE 1) can be contracted later in life--a
fact too often overlooked by seniors and health care providers alike. Recent
research has provided evidence that many older adults are sexually active;
however, seniors know less about STDs and HIV/AIDS than younger individuals
because the elderly have been neglected by those responsible for education and
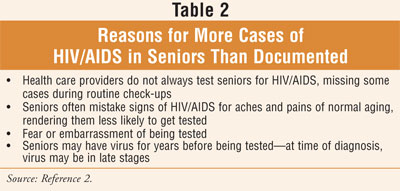
prevention messages.1,2 While it is estimated that 19% of all
people with HIV/AIDS in this country are age 50 and older, the National
Institute on Aging reports that there are more cases in seniors that go
undocumented (TABLE 2).2 Clinicians are discovering HIV in
seniors in growing numbers compared with previous years, and the number of
older adults infected with HIV is expected to rise as baby boomers continue to
age.2,3
Sexual Activity and the
Older Adult
Active sexuality
continues in a rather high proportion of men and women in advanced age.4
A national representative study found the majority of older adults (ages
57–85) are engaged in spousal or other intimate relationships and regard
sexuality as an important part of life.1 Reported sexual activity
included vaginal intercourse, oral sex, and masturbation; activity did decline
with age.1 The researchers noted that physical health is more
strongly associated with many sexual problems than age alone.1
Among women studied, the most prevalent sexual difficulties included low
desire (43%), difficulty with vaginal lubrication (39%), and inability to
climax (34%); among men, erectile difficulties prevailed (37%).1
This particular study confirmed prior re search indicating that diabetes is
positively associated with erectile dysfunction, as well as a lower prevalence
of sexual activity with a partner and masturbation.1 Sexual
problems among seniors are not frequently discussed with physicians, even
though they may be a warning sign or consequence of a serious underlying
illness (e.g., cancer, diabetes, infection, urogenital tract condition).1,5,6
When undiagnosed or left untreated, sexual problems can precipitate or
co-exist with depression or social withdrawal.1,7-9 It
should not be overlooked that patients may, and often do, discontinue required
medicationssecondary to adverse effects that affect their sexual activity.1
Changes in social norms (e.g.,
dating, divorce, sex) and the huge market for medications and devices for the
treatment of sexual problems targeting older adults facilitate more active sex
lives.1,10 Early in the HIV epidemic, most HIV-acquired infections
in seniors were secondary to blood transfusions.11 Since the
introduction of donor screening, however, transmission by this route has
decreased dramatically.11 Today, HIV infection in seniors is most
commonly transmitted through sexual activity.11 Researchers studied
the sexual behavior of self-identified gay men between the ages of 25 and 77.10,12
The study found that 44% of men older than 60 had multiple partners, virtually
equal to the number in the 30 to 39 age group.10,12 Fewer older men
were in long-term relationships with other men, and younger men were more
likely to have engaged in a broader range of sexual activities, including
receptive anal intercourse.10,12
Seniors are less likely than
younger people to talk about their sex lives or drug use with their
physicians, and physicians tend not to ask older patients about these
activities.2 Older adults often mistake the symptoms of HIV/AIDS
for the aches and pains of normal aging, so they are less likely to get tested.2
The clinician faces challenges such as distinguishing among those conditions
that are age related, those that are HIV related, those that are not
distinguishable, and those related to both.10,13 Symptoms like
shortness of breath, fatigue, chronic pain, and weight loss are often
associated with HIV disease.10 While physiologic differences among
age groups contribute to STD susceptibility (i.e., two-thirds of STD cases
occur in teens and those in their twenties), aging is associated with
physiologic changes that increase the risk of any infection, including
STDs.3,11 Compared with younger people, the aging adult may be at
higher risk for progression to AIDS according to some research; this is
certainly the case for seniors with low T-cell counts.10 Overall,
there is an abundance of evidence supporting the need for transmission
prevention in seniors.
Risk Factors
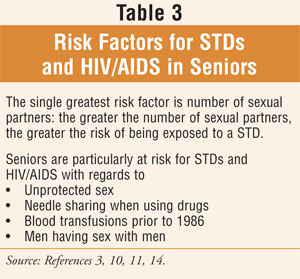
The single greatest
risk factor for STDs is number of sexual partners: the greater the number of
sexual partners, the greater the risk of being exposed to a STD.14
Factors placing seniors particularly at risk for STDs and HIV/AIDS are given
in TABLE 3. The fact that seniors are one-sixth less likely to use
condoms than people in their twenties underscores the risk factor of
unprotected sex in this population.11 Sexual preference plays an
important role in the transmission of STDs as well. Disproportionately greater
rates of STDs occur in men having sex with men (MSM) with respect to multiple
partners and unprotected anal-genital, oral-genital, and oral-anal intercourse.4,14
The literature has revealed senior women in particular seem to be uninformed
about the transmission and risks of HIV.10
Screening
Screening for STDs
is an essential part of health care for sexually active men and women.15,16
Furthermore, omitting seniors from the screening process increases the risk
that by the time seniors are diagnosed with HIV/AIDS, the virus may be in the
late stages.2 Recently, federal officials noted that many cases of
STDs (e.g., syphilis, gonorrhea, chlamydia) are escaping detection because MSM
are not being tested each year as advised.15,16 Evidence from CDC
research shows that among MSM who showed no symptoms of gonorrhea, rectal
infections (more than one-third) and throat infections (more than one-quarter)
were missed since many individuals were not tested at all anatomical sites of
recent exposure.15 Up-to-date screening guidelines that include
recommendations for the screening of sexual partners are available online.16
Prevention
Sexually active persons can reduce risk of transmitting and acquiring STDs and HIV/AIDS by: 1) adopting safer sexual behaviors; 2) using male/female condoms (latex or polyurethane); 3) having partners tested for HIV; and 4) avoiding sharing needles or any other equipment used to inject drugs.10,11,14 Testing should be done if a senior or partner had a blood transfusion between 1978 and 1985 and/or has had an operation or blood transfusion in a developing country at any time.10 An overview of measures for the prevention and control of STDs and HIV/AIDS can be found in TABLE 4.
![]()
Treatment Update
Most STDs are easily cured with
antibiotics, except for viral STDs (e.g., genital herpes, HPV, HIV), which are
symptomatically treated by palliative and suppressive therapy.4,16
Current recommendations for HIV treatment advocate a minimum of three
antiretroviral agents (e.g., two nucleoside analogues with either a protease
inhibitor [usually enhanced with ritonavir] or a nonnucleoside) referred to as highly
active antiretroviral therapy (HAART).16,17 The goal is to use
potent combinations of antiretroviral agents to maximally inhibit viral
replication and restore immune function.3,17 Drug–drug interactions
with HIV antiretroviral therapy may be found in Reference 18.
The CDC no longer recommends
the use of fluoroquinolones for the treatment of gonococcal infections and
associated conditions such as pelvic inflammatory disease.3,16,18
Consequently, only one class of drugs, the cephalosporins, is still
recommended for the treatment of gonorrhea.3,16,19 The
third-generation cephalosporin, ceftriaxone 125 mg IM in a single dose, is the
preferred regimen according to the CDC for all types of uncomplicated
gonococcal infection (i.e., genital, anal, pharyngeal).16 In
geriatric patients, no dosage adjustment is required for renal impairment.20
Nonadherence to multiple-dose regimens results in treatment failures for most
STDs; single-dose therapies when appropriate may improve patient adherence.3
Although it is beyond the scope of this article to discuss the pharmacologic
treatment of STDs and HIV/AIDS in detail, the reader is encouraged to refer to
Reference 16 for CDC's online STD Treatment Guidelines, which includes
alternative regimens and recommendations for the treatment of sexual partners.
Pharmacists should make recommendations for renal and hepatic dosing when
appropriate for safe and effective treatment and optimal therapeutic outcomes.
Conclusion
Sexual activity and
the potential for STDs continue into late life. Sexual dysfunction is
associated with poor health and may adversely affect adherence to necessary
medication. A confluence of factors, including changes in demographics and
social norms, and HAART extending lives, requires increased attention to the
impact of STDs and HIV/AIDS among seniors.2,10 Pharmacists should
raise awareness and promote the appropriate screening, treatment, and
prevention of STDs in this vulnerable population. There is a current and
future role for pharmacists in recognizing and preventing drug interactions in
seniors with HIV/AIDS and providing recommendations to health care providers
regarding the most current guidelines for the treatment and management of STDs.
REFERENCES
1. Lindau ST, Schumm LP, Laumann EO, et al. A study of sexuality and health among older adults in the United States. N Engl J Med. 2007;357:762-774.
2. Age Page: HIV, AIDS, and older people. National Institute on Aging. www.nia.nih.gov/HealthInformation/Publications/hiv-aids.htm. Accessed July 7, 2008.
3. Zagaria ME. The aging population and sexually transmitted diseases. Presented at: American Society of Consultant Pharmacists Midyear Conference; May 16, 2008; Las Vegas, NV.
4. Zagaria ME. Sexually transmitted diseases in older patients. US Pharm. 2003;23(12):26-29.
5. Isselbacher KJ, Martin JB, Braunwald E, et al, eds. Harrison's Principles of Internal Medicine. 13th ed. New York, NY: McGraw-Hill, Inc; 1994:262.
6. Rosen RC, Wing R, Schneider S, Gendrano N. Epidemiology of erectile dysfunction: the role of medical comorbidities and lifestyle factors. Urol Clin North Am. 2005;32:403-417.
7. Nicolosi A, Moreira ED Jr, Villa M, Glasser DB. A population study of the association between sexual function, sexual satisfaction and depressive symptoms in men. J Affect Disord. 2004;82:235-243.
8. Morley JE, Tariq SH. Sexual dysfunction in older persons. In: Hazzard WR, Blass JP, Halter JB, et al, eds. Principles of Geriatric Medicine and Gerontology. 5th ed. New York, NY: McGraw-Hill, Inc; 2003:1311-1323.
9. Araujo AB, Durante R, Feldman HA, et al. The relationship between depressive symptoms and male erectile dysfunction: cross-sectional results from the Massachusetts Male Aging Study. Psychosom Med.1998;60:458-465.
10. HIV disease in individuals ages
fifty and above. Health Resources and Services Administration. U.S. Department
of Health and Human Services. February 2001. http://hab.hrsa.gov/
publications/hrsa201.htm.
Accessed July 14, 2008.
11. Beers MH, Berkow R, eds. The Merck Manual of Geriatrics. 3rd ed. Whitehouse Station, NJ: Merck & Co.; 2000:1357-1359,1378-1382.
12. Slusher MP. Patterns of sexual behavior among younger and older gay men. Presented at: Gerontological Society of America Scientific Meeting; November 18-22, 1994; Atlanta, GA.
13. Linsk NL. HIV among older adults: age-specific issues in prevention and treatment. AIDS Read. 2000;10:430-440.
14. Knodel LC. Sexually transmitted diseases. In: DiPiro JT, Talbert RL, Yee GC, et al, eds. Pharmacotherapy: A Pathophysiologic Approach. 6th ed. New York, NY: McGraw-Hill, Inc; 2005:2097-2117.
15. Sex diseases in many gay men go unfound, experts say. New York Times. March 12, 2008:A21.
16. STD Treatment Guidelines 2006. The Centers for Disease Control and Prevention (CDC). Updated April 2007. www.cdc.gov/std/treatment/. Accessed March 16, 2008.
17. Howland RD, Mycek MJ. Pharmacology. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2006:433-452.
18. Clark A, Stein CR, Townsend ML.
Drug-drug interactions with HIV antiretroviral therapy. US Pharm.
2008;33(4):HS3-HS21. www.uspharmacist.com/index.asp?show=article&page=
8_2265.htm. Accessed
May 1, 2008.
19. Update to CDC's Sexually Transmitted Diseases Treatment Guidelines, 2006: fluoroquinolones no longer recommended for treatment of gonococcal infections. April 13, 2007. www.cdc.gov/mmwr/preview/mmwrhtml/mm5614a3.htm?s_cid=mm5614a3_e. Accessed March 15, 2008.
20. Semla TP, Beizer JL, Higbee MD. Geriatric Dosage Handbook. 12th ed. Hudson, OH: Lexi-Comp, Inc; 2007:267.
21. Beers MH, Porter RS, Jones TV, et al. The Merck Manual of Diagnosis and Therapy. 18th ed. Whitehouse Station, NJ: Merck Research Laboratories; 2006:1650-1664.
To comment on this article, contact rdavidson@jobson.com.



