US Pharm. 2007;32(4):38-46.
Topical isotretinoin (Retin-A) was introduced to the market in the early 1970s. In 1979, the FDA approved the oral formulation of isotretinoin (Accutane) for the treatment of nodulocystic acne. Since then, oral isotretinoin has been studied as therapy for several types of cancer, such as chemoprophylaxis of squamous cell carcinoma of the skin and certain types of leukemia. The oral formulation has also been used in other diseases, including cutaneous lupus, psoriasis, and rosacea.1 Among the several different mechanisms of isotretinoin, a naturally occurring metabolite of vitamin A, are that it reduces sebaceous gland size and sebum production and regulates cell proliferation and differentiation.2
Many physicians are wary of prescribing isotretinoin based on its teratogenic effects and the potential liability associated with its use. In order to reduce fetal exposure to isotretinoin, the FDA approved iPLEDGE, a risk management program to regulate the use of isotretinoin, on March 1, 2006. iPLEDGE replaced the manufacturer-initiated SMART (System to Manage Accutane Related Teratogenicity) program and is now the only way pharmacists can dispense isotretinoin. The goals of iPLEDGE are to ensure that women using isotretinoin do not become pregnant and that women who are pregnant do not use isotretinoin.
In addition to concerns regarding fetal abnormalities, there continues to be controversy over the possible role of isotretinoin in causing suicide and depression. This issue warrants heightened precautions by prescribers. To achieve the safest and most beneficial outcome for the patient taking isotretinoin, it is important to adhere to the manufacturer's prescribing information.
Toxic Effects
Although isotretinoin is a toxic drug, when prescribed and monitored
appropriately, it can provide major improvement to patients with cystic acne.
However, isotretinoin can also cause mucocutaneous, ophthalmologic,
gastrointestinal, neuromuscular, psychiatric, and rheumatologic side effects,
in addition to laboratory and fetal abnormalities.1
Some minor side effects of isotretinoin are cheilitis, occurring in 91% of patients, and dry mouth, which affects 80% of patients. Ninety percent of patients who report adverse effects of the skin and subcutaneous body tissue experience dry skin, localized exfoliation, erythematous rash, and dermatitis. The incidence of these effects tends to increase within the first four weeks of therapy and then declines at around 12 to 16 weeks. Near week four of therapy, dry skin and facial rash typically occur, often accompanied by an acne flare.3 Dry eyes and nosebleeds are also very common complaints, especially during the first eight weeks.1 Patients who wear contact lenses will often have to remove them because of discomfort. In addition, patients may experience impaired night vision.3
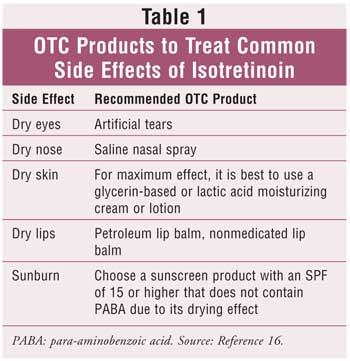
Cheilitis can be relieved with topical emollients, lubricants, or low-dose steroids. Vitamin E (800 IU/day) has been studied to treat such side effects as alopecia and cheilitis but has not been shown to be clinically effective.1 A lotion or emollient with sunscreen should be recommended to patients at the initiation of therapy. Table 1 includes recommended OTC products for the treatment of common adverse effects. Other minor side effects include headache (5%), transient alopecia (10%), and myalgias (15%).1,3
Major toxic effects of isotretinoin include pseudotumor cerebri (with the use of tetracycline), pancreatitis, lipid disorders, hearing impairment, hepatotoxicity, inflammatory bowel disease, vision impairment, and a decrease in bone mineral density.4 Isotretinoin causes an elevation of aspartate aminotransferase (AST), alanine aminotransferase (ALT), and lactate dehydrogenase (LDH) in 15% of patients. Triglyceride levels can rise in 25% of patients and can lead to pancreatitis. 1 Blood dyscrasias such as neutropenia, anemia, and agranulocytosis have also been linked to isotretinoin.2 Specific birth defects associated with isotretinoin include cardiovascular effects such as Tetralogy of Fallot and ventricular septal defects. In addition, facial dysmorphia, cleft palate, microphthalmia, microcephaly, and hydrocephalus have occurred. It has been reported that over half of children exposed to the drug in utero experience intellectual defects.9
Monitoring
Oral isotretinoin causes a mild, usually reversible, elevation of liver
function tests.1,5 Therefore, monitoring is essential to ensure
safe use of the product. It is recommended that baseline and weekly or
biweekly liver function tests be obtained until the response to therapy is
established, which is usually four weeks after beginning treatment.6
Mild elevations in liver enzymes less than twice the upper limit of normal
occur in 15% to 25% of patients. In these cases, therapy can be continued, but
laboratory results should be closely monitored. If patients experience an
elevation in liver enzymes greater than twice the upper limit of normal,
isotretinoin should be discontinued or the dosage should be lowered.7
Patients taking isotretinoin are also at risk for hyperlipidemia, especially
those with elevated triglyceride levels.1 A pretreatment lipid
panel and follow-up monitoring at weekly or biweekly intervals are necessary
for the first four weeks of therapy. The lipid panel should be drawn at least
36 hours after any alcohol consumption in order to prevent detection of
falsely elevated enzymes.6 If patients experience mild
hypertriglyceridemia (?400 mg/dL), they should modify their diet and
reduce alcohol intake.4 If patients have triglyceride levels of 800
mg/dL or higher, therapy should be discontinued or the dosage should be
lowered. Patients who experience signs or symptoms of pancreatitis should stop
therapy immediately. Lipid elevations usually decline several weeks after
decreasing the dosage of isotretinoin.7 Because several blood
dyscrasias have been reported, including a case of severe thrombocytopenia,
8 a complete blood count should be obtained before and throughout
treatment for optimal safety. There is no consensus on the frequency of
monitoring this parameter.5
Pregnancy Tests
Since isotretinoin is associated with many birth defects, e.g.,
cardiovascular, craniofacial, thymus, and central nervous system effects, it
is considered pregnancy category X.9 Therefore, the FDA requires
that all women of childbearing age be given a monthly pregnancy test while
taking isotretinoin.6 In order to initiate therapy, the
manufacturer recommends two negative serum or urine pregnancy tests; the
second must be done in a CLIA (Clinical Laboratory Improvement
Amendments)-certified laboratory. For those women with regular menstrual
cycles, the first test should be performed when the decision is made to begin
therapy and the second during the first five days of the menstrual period
prior to starting isotretinoin. The second test should also be performed
within seven days of the office visit and after using two forms of birth
control for one month.4 The serum test should have a sensitivity of
at least 25 mIU/mL.4 The test results must be entered into the
iPLEDGE system within seven days. Results must be negative in order for a
prescription to be authorized. A pregnancy test must also be obtained after
the last dose of isotretinoin is administered and one month later.10
All women should be educated about the risks of isotretinoin and required to use two forms of contraception, starting one month prior to therapy and continuing for one month posttherapy.4,9 Recommended primary forms of birth control include tubal sterilization, vasectomy, intrauterine device, and combination hormonal therapy. Secondary forms of contraception include condoms, diaphragms, cervical caps, and vaginal sponges containing spermicide. Patients should be educated about appropriate forms of birth control, since some forms are unacceptable, such as the female condom and progesterone-only birth control pills.10 A low level of isotretinoin can be detected in the semen of males taking isotretinoin; however, a cause-and-effect relationship between birth defects and drug in the semen has not been established.4
Psychiatric Illness
A controversy surrounding the use of isotretinoin has been its potential with
psychiatric disorders in adolescents, including depression and suicide. Oral
isotretinoin has been a questionable source of psychiatric illness in over 400
cases since its introduction on the market.11 Currently, there is
insufficient evidence to causatively link isotretinoin to these psychiatric
conditions.5,11 However, in a number of the cases, the disorder
subsided with discontinuation of therapy and resumed once therapy was
restarted.12 It has been suggested that acne itself may be the
cause of these disorders.5,11 Suicide is one of the major causes of
death in people 15 to 34 years old, which coincides with the age group most
likely to use isotretinoin.5 The package insert contains a warning
stating that isotretinoin may cause depression, psychosis, and violent
behavior, but rarely suicide or suicidal ideations.4 Patients
should be evaluated prior to starting therapy, and those with any type of
mental illness should be monitored closely during therapy.5 Parents
of children prescribed isotretinoin should be informed of the potential
psychiatric side effects and symptoms to monitor for, such as depression,
psychosis, and violent behavior.
Drug Interactions
Isotretinoin is eliminated in the urine and feces in equal amounts and is
metabolized hepatically. Fortunately, there are few documented drug
interactions. Isotretinoin may decrease carbamazepine levels and may interfere
with the efficacy of progesterone-only birth control pills. Patients should
avoid supplements containing vitamin A due to possible toxicity. Tetracyclines
should be avoided, since concomitant use has been implicated in the
development of pseudotumor cerebri.2,4
Dosage and Administration
Isotretinoin is available in brand (Accutane) and generic form (Amnesteen,
Clavaris, and Sotret) in 10-, 20-, and 40-mg capsules. The dosage for severe
recalcitrant nodular acne is 0.5 to 2 mg/kg in two divided doses per day. The
recommended dose for children 13 to 17 years old is 1 mg/kg divided into two
daily doses.6 Cumulative doses range from 120 to 150 mg/kg over a
four- to six-month period. Greater efficacy and decreased relapse rates have
been associated with higher individual (>1 mg/kg/day) and cumulative doses.
13 Treatment should continue for 15 to 20 weeks or until the total cyst
count decreases by 70%, depending on what comes first. A second course of
therapy may be started once the patient has been off treatment for at least
two months.2 Patients taking isotretinoin should avoid alcohol,
prolonged exposure to sunlight and UV rays, and be informed that they cannot
donate blood for at least one month after they stop taking the drug.2
The iPLEDGE Program
Prior to 2006, the SMART program was launched in April 2002. This FDA-approved
program, provided by the manufacturer, was used to decrease the number of
teratogenic events caused by exposure to isotretinoin. The FDA and
manufacturers of both brand and generic formulations of isotretinoin have
since approved the iPLEDGE program in an effort to reduce fetal exposure to
the drug and to prevent pregnancy during use. The iPLEDGE program is more
stringent than SMART in its requirements for dispensing isotretinoin and
implements the use of a computer-based system to track information related to
the drug. Wholesalers, prescribers, pharmacies, and patients must register
with the system in order to distribute, prescribe, dispense, or use
isotretinoin and must reactivate their registration annually. The iPLEDGE
program tracks the use of isotretinoin from wholesaler to prescriber and then
to the patient.
Unfortunately, with all of the available resources, isotretinoin is still being misprescribed.14 Prescribers must ensure that patients meet the criteria for isotretinoin use and document this information in the system every month that the patient is prescribed isotretinoin. Prescribers must document two forms of contraception used by the patient, pregnancy test results, and confirmation of patient counseling. Patients are responsible for also documenting their two types of contraception and correctly answering questions about pregnancy prevention and the iPLEDGE system. Unlike the SMART program, which only allows written prescriptions, iPLEDGE enables prescriptions to be given by phone, fax, or e-mail.10 Additional information for pharmacists regarding the iPLEDGEprogram is provided in Table 2.

Initially, patients taking isotretinoin were not allowed to qualify for their next prescription until 23 days after the end of their seven-day window, regardless of whether they had their prescription filled. In October 2006, this rule was updated to allow male patients and female patients of non-childbearing age to have a prescription filled after their seven-day window expired. The seven-day window begins once a patient has been counseled in the physician's office and the prescription is written. 10 All patients must still undergo the qualification process with each prescription. (Pharmacists can access the program at www.ipledgeprogram.com or by phone at 1-866-495-0654.) The manufacturer recommends that all patients sign a consent form before initiating therapy. This form is available in the package insert.3 Any cases of pregnancy should be reported to MedWatch, the FDA's adverse events program.2
A possible disadvantage to the iPLEDGE system is an increased workload for the physician and pharmacist to dispense and prescribe the drug. This disadvantage may result in patients who could benefit from the product not receiving it.
In March 2007, the FDA launched a Web page (www.fda.gov/buyonline/accutane) warning about the dangers of buying isotretinoin online. The new Web page appears in online search results for the brand or generic versions. The page emphasizes that the drug be taken only under the supervision of a physician or pharmacist and provides links to helpful information.
Isotretinoin can be a valuable, efficacious drug in the treatment of acne and is safe for patients if all procedures are followed appropriately and patients are monitored closely. Proper use of isotretinoin is dependent on the physician and pharmacist to properly educate patients on the risks of isotretinoin. Since 1982, there have been over 1,995 documented cases of pregnant women exposed to isotretinoin. With the low rate of reporting and enrollment in the SMART program, this number could be a great underrepresentation.15 The iPLEDGE program will hopefully decrease the number of fetal exposures to isotretinoin and enable providers and pharmacists to feel more at ease prescribing and dispensing the product.
References
1. Sekula-Gibbs S, Uptmore D, Otillar L. Retinoids. J Am Acad Dermatol.
2004;50:405-415.
2. Drug Information Handbook. Hudson, OH: LEXI-COMP; 2006.
3. McLane J. Analysis of common side effects of isotretinoin. J Am Acad
Dermatol. 2001;45:S188-S194.
4. Accutane package insert. Roche Laboratories, Inc., Nutley, NJ; 2000-2005.
5. Goldsmith LA, Bolognia JL, Callen, JP et al. American Academy of
Dermatology Consensus Conference on the safe and optimal use of isotretinoin:
Summary and recommendations. J Am Acad Dermatol. 2004;50:900-906.
6. Micromedex. Montvale, NJ: Thomson Healthcare. vol. 122. 1974-2006.
7. Koda-Kimble MA, Young LY. Applied Therapeutics: The Clinical Use of Drugs
. 7th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2001:37-9-37-10.
8. Moeller KE, Touma SC. Prolonged thrombocytopenia associated with
isotretinoin. Ann Pharmacother. 2003;37:1622-1624.
9. Chan A, Hanna M, Abbott M, et al. Oral retinoids and pregnancy. MJA.
1996;165:164-167.
10. The iPLEDGE program guide to best practices for isotretinoin. Available
at: www.ipledgeprogram.com. Accessed December 12, 2006.
11. Enders SJ, Enders JM. Isotretinoin and psychiatric illness in adolescents
and young adults. Ann Pharmacother. 2003;37:1124-1127.
12. Mangin P, Pond D, Smith W. Isotretinoin, depression, and suicide: a review
of the evidence. Br J Gen Pract. 2005;134-138.
13. Haider A, Shaw JC. Treatment of acne vulgaris. JAMA.
2004;292:726-735.
14. The iPLEDGE pharmacist guide. Available at:
www.nacds.org/user-assets/PDF_files/Final%20Pharmacist%20Guide.pdf. Accessed
November 16, 2006.
15. Jones KL, Adams J, Chambers CD, et al. Isotretinoin and pregnancy. JAMA
. 2001;285:2079-2080.
16. Berardi RR, Kroon LA, et al. Handbook of Nonprescription Drugs: An
Interactive Approach to Self-Care. 15th ed. Washington, D.C.: American
Pharmacists Association; 2006.
To comment on this article, contact editor@uspharmacist.com.


