US Pharm. 2006;31(11)(Diabetes suppl):1-4.
With
the rising number of patients opting for alternative therapies, it behooves
health care practitioners to learn more about the value of these approaches.
It is increasingly important for physicians, pharmacists, and other providers
to have a working understanding of how essential nutrients promote health and
prevent disease. There is no greater need for such a comprehensive approach
than in metabolic health, given the sharp rise in the past 25 years in the
number of people with diabetes and those at risk.1 The learning
curve starts with an understanding of the basic building blocks that promote
metabolic health, particularly insulin health and glucose metabolism. This
article reviews recent studies on two essential nutrients--chromium and
biotin--and their beneficial effects on glycemic control.
Chromium is an essential trace
mineral required by the human body for normal carbohydrate and lipid
metabolism.2 The body cannot make chromium; it must be obtained
through the diet or by supplementation. The U.S. Department of Agriculture's
analysis of food intake data suggests that the average American diet is low in
chromium.3 Anderson reported that dietary intake of chromium is
suboptimal in the U.S.3 Nutritional chromium is found in minute
quantities in foods such as organ meats, oysters, mushrooms, broccoli, and
brewers' yeast, and is further compromised by modern food processing and
cooking methods. Rising sugar consumption also reduces chromium reserves in
the body. Finally, aging is associated with a 25% to 40% drop in tissue
chromium and may be implicated in type 2 diabetes mellitus (T2DM).4
Research indicates that diets
containing less than 25% of normal chromium levels adversely affect insulin
sensitivity in subjects with mildly impaired glucose tolerance. Over time,
chromium loss may contribute to insulin resistance or may exacerbate it in
people with T2DM.3
Chromium picolinate (CrPic) is
an excellent source of chromium, since it is better absorbed and utilized by
the body than is chromium chloride or other forms of nutritional chromium.
Daily supplementation with 200 to 1,000 mcg of chromium as CrPic has
consistently been found to improve insulin sensitivity, glucose tolerance, and
circulating insulin levels.2,3 Of 13 human studies investigating
CrPic's effectiveness in improving glucose control, 12 have shown significant
positive effects in patients with type 1, type 2, and gestational diabetes, as
well as in those at risk for diabetes.2,3
Biotin, a member of the B
vitamin complex, is necessary for both metabolism and growth in humans,
particularly in the production of fatty acids, antibodies, and digestive
enzymes and in tissue metabolism.5 Importantly, for patients with
diabetes, biotin stimulates liver glucokinase activity, increases insulin
production, and enhances glucose uptake in muscle cells.6-8 Food
sources of biotin include organ meats, soy, egg yolks, whole grains, and
yeast. There is growing evidence of suboptimum biotin intake in the U.S.
population.9
Preclinical Studies
The following data
are presented to support the beneficial effects of a supplement containing
CrPic and biotin.
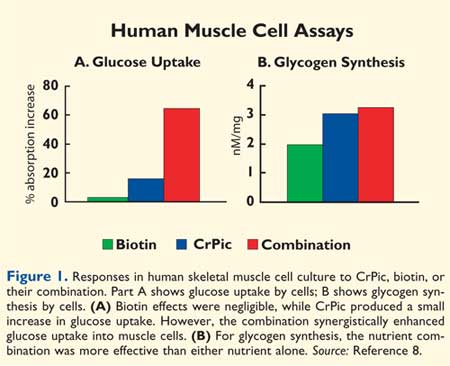
Increased Glucose
Uptake: Researchers
from University of Vermont incubated human skeletal muscle cell with
CrPic, biotin, or a combination of these. The combination enhanced glucose
uptake and increased glycogen synthesis through elevated glycogen synthase
levels (Figure 1).8 A deficiency in glycogen synthase may
lead to hyperglycemia and may contribute to insulin resistance.
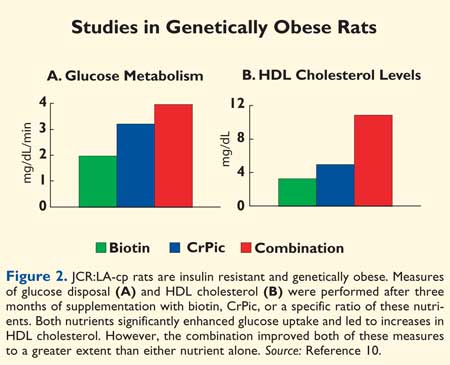
Improved Glucose
Metabolism and HDL Cholesterol Levels:
JCR:LA-cp rats, a genetically obese, insulin-resistant animal model, were
given CrPic and biotin combined or separately. This animal model exhibits many
cardiovascular risk factors seen in obese humans. All nutrients, except for
the lowest CrPic dose, significantly raised HDL cholesterol (HDL-C) levels.
The highest doses of CrPic/biotin worked synergistically to increase HDL-C and
improved glucose metabolism beyond that of either nutrient alone (Figure 2
).10 Researchers hypothesized that the combination might benefit
people who are insulin resistant and at risk for cardiovascular disease (CVD).
Importantly, some combinations
of CrPic and biotin were more effective than others and were defined in these
preclinical studies prior tohuman clinical trials.10
Human Clinical Studies
Improved
Glycosylated Hemoglobin Levels:
A 447-patient, double-blind, placebo-controlled study was conducted examining
the impact of CrPic and biotin on glycemic control and lipid profile in
patients with T2DM.11 Subjects had hemoglobin A1C (HbA1c) levels of
7% or higher, were taking stable oral antidiabetic medications for at least 60
days, had a body mass index more than 25 and less than 35 kg/m2,
and had at least a one-year history of T2DM. Subjects received CrPic/biotin or
placebo for 90 days. They continued therapy with their current oral
antidiabetic agent(s) throughout the study.
A total of 369 subjects
completed at least one follow-up visit. Of this population, those taking
CrPic/biotin showed significant improvements in their levels of HbA1c (P
<.01) and total cholesterol (TC) (P <.02) and in their
triglycerides (TG)/HDL-C ratio (P <.0001), compared to placebo
recipients. The greatest improvement in HbA1c levels occurred in subjects with
the highest baseline HbA1c levels. For example, subjects whose baseline HbA1c
level was above 10% averaged a 1.78-percentage point decrease, and those whose
level was above 11% averaged nearly a 2–percentage point drop. In this
high-risk group, the proportion of subjects with a 1–percentage point relative
reduction from baseline was significantly higher in the CrPic/biotin group
(74%) than in the placebo group (39%). Thus, CrPic/biotin may benefit
individuals with T2DM who are hyperglycemic and have dyslipidemia, by reducing
risk factors.
As a follow-up to this
clinical trial, an open-label study followed 24 subjects taking CrPic/biotin
along with their diabetes medications for another nine-month period. The mean
HbA1c dropped significantly (-1.07%, P <.0001). Ten of 24 subjects
reached the target of 7% established by the American Diabetes Association.
This long-term study demonstrated the safety and effectiveness of the
combination for the treatment of T2DM.
Improved Postprandial
Glucose Levels:
In a 30-day, double-blind, placebo-controlled study, 36 subjects with
persistent impaired glucose control (two-hour glucose > 200 mg/dL) and HbA1c
level at or above 7% and with at least a one-year history of T2DM were
randomized to receive CrPic/biotin or placebo.12 Results showed a
significant decrease in area under the curve for glucose (two-hour oral
glucose tolerance test: P <.03), TG (P<.03), and TG/HDL-C (
P <.05) between groups. A significant correlation was noted between body
weight and lipids (P<.05) and in the homeostasis model assessment for
insulin resistance (P<.03) in the active group but not in the placebo
group. In addition, a highly significant decrease in TC/HDL-C (P <0.03)
and LDL-C/HDL-C (P <.05) was observed between groups. Consistent with
its impact on impaired glucose control and coronary risk factors, CrPic/biotin
improved insulin sensitivity and may therefore be a useful and cost-effective
adjuvant therapy to improve impaired glucose tolerance.
Improved Glycemic
Control: In an
intervention program called the Diachrome Patient Experience Program (PEP),
more than 100 participants with T2DM were tested. Patients worked with
diabetes educators, received educational literature, were instructed in the
use of a home blood glucose monitor, and received supplements containing
CrPic/biotin. Participants continued their prescription antidiabetic
medications.
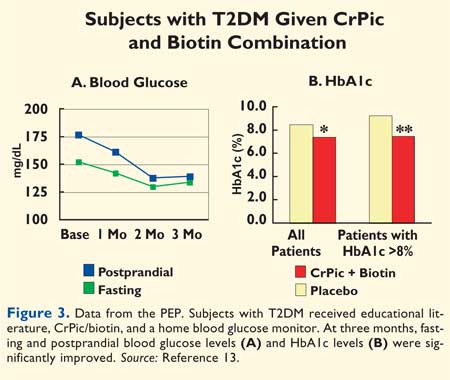
The PEP aimed to evaluate
whether CrPic/biotin could reduce elevated HbA1c levels when used in a "real
life uncontrolled environment" in people with T2DM. Participants received
CrPic/biotin for 12 weeks. Overall, the study found significant improvements
in fasting and postprandial blood glucose levels, as well as lowered HbA1c
levels. The average drop in fasting blood glucose (FBG) levels was from 158 to
137 mg/dL (P <.05), with an average drop of postprandial readings from
191 to 163 mg/dL (P<.01; Figure 3A).13 Significant
changes in postprandial levels were seen within the first month, while
significant lowering of fasting levels was seen at 90 days.
A separate analysis was
performed of subjects (n = 30) whose HbA1c levels were highly elevated (>7%)
despite the use of oral hypoglycemic agents. In these subjects, a reduction of
1.1 percentage points in average HbA1c (from 8.5% to 7.4%; P <.005) was
seen. Eighteen participants with baseline HbA1c levels above 8% showed an
average decrease of 1.8 percentage points (from 9.3% to 7.5%; P<.001) (
Figure 3B). Thus, the greatest improvements were observed in patients with
the highest baseline levels (P<.001).13
Improved Lipid and
Lipoprotein Levels:
In the 90-day, double-blind, placebo-controlled study in people with T2DM
referenced above, a subset of patients with high cholesterol levels (>200
mg/dL) taking CrPic/biotin showed improved blood lipid profiles, including
reduced LDL (P <.02) and TC levels (P<.02).11,14
In addition, subjects with elevated non–HDL-C levels (>130 mg/dL) taking
CrPic/biotin experienced reductions in TG (225 vs. 278 mg/dL), TG/HDL-C (5.4
vs. 6.6), TC/HDL-C (4.5 vs. 5.0), very low-density lipoprotein (VLDL)-C (37
vs. 49 mg/dL), and LDL-C/TG (0.79 vs. 0.66), compared to placebo recipients.
The atherogenic index (AI = log[Tg/HDL]), a surrogate marker for CVD risk, was
significantly reduced (P <.04) in active subjects, compared to placebo
recipients. Thus, diabetic patients with elevated cholesterol can obtain
significant improvement in lipid and lipoprotein levels after taking
CrPic/biotin.
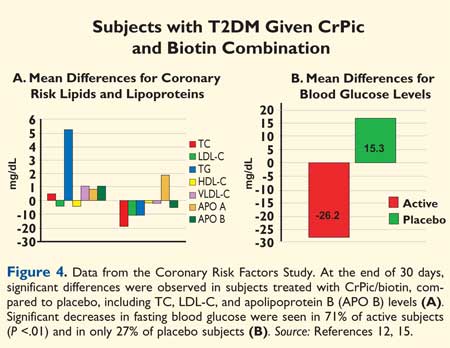
Another controlled study
included subjects with two-hour glucose levels above 200 mg/dL on stable oral
antidiabetic medications, HbA1c levels higher than 7%, and at least a one-year
history of T2DM. Subjects were placed on CrPic/biotin (n =13) or placebo (n =
11). During a 30-day period, decreases in FBG, lipids, and lipoproteins were
observed. Subjects treated with CrPic/biotin experienced significant decreases
in TC (-19.1 mg/dL; P <.03), LDL-C (-10.9 mg/dL; P<.01) and
apolipoprotein B (-5.3 mg/dL; P<.03) levels, while placebo recipients
experienced increases in these measures (Figure 4).12,15
Conclusion
Mounting clinical evidence supports
the efficacy of CrPic/biotin for improving parameters of blood glucose
utilization, insulin sensitivity, and lipid metabolism in patients with
diabetes. Based on clinical results, dosing is recommended in a single daily
capsule containing 600 mcg of chromium (as CrPic) plus 2 mg of biotin, taken
in the morning preferably.
Proposed mechanisms for the
nutrient combination suggest an enhancement of glucose disposal, glycogen
synthesis, and increased glycogen synthase levels in skeletal muscle, with
major implications in insulin resistance.
A 30-day rapid response to
this nutrient formulation has been demonstrated in controlled studies
measuring FBG and coronary risk factors. Longer-term (90-day) studies have
shown additional improvements in HbA1c levels. Improvements in glycemic
control, coupled with reductions in coronary risk factors, suggest that this
product holds promise for longer-term impact in people with diabetes.
This nutritional adjuvant
therapy offers promise for many of today's most critical health concerns
linked to insulin resistance, including diabetes, impaired glucose tolerance,
and metabolic syndrome. To better manage patients with T2DM, the addition of
CrPic/biotin should be considered as part of first-line treatment, in addition
to lifestyle modification and longer-term adjuvant therapy.
CrPic/biotin is available as
Diachrome from Nutrition 21, Inc.
References
1. Centers for Disease Control and
Prevention. Data & Trends: Prevalence of Diabetes. Available at:
www.cdc.gov/diabetes/statistics/prev/national/figpersons.
htm. Accessed October 2, 2006.
2. Cefalu WT, Hu FB. Role of chromium in human health and in diabetes. Diabetes Care. 2004;27:2741-2751.
3. Anderson RA. Chromium in the prevention and control of diabetes. Diabetes Metab. 2000;26:22-27.
4. Davies S, McLaren Howard J, et al. Age-related decreases in chromium levels in 51,665 hair, sweat, and serum samples from 40,872 patients: implications for the prevention of cardiovascular disease and type II diabetes mellitus. Metabolism. 1997;46:469-473.
5. Dakshinamurti K, Tarrago-Litvak L, Hong HC. Biotin and glucose metabolism. Can J Biochem. 1970;48:493-500.
6. Dakshinamurti K, Cheah-Tan C. Biotin-mediated synthesis of hepatic glucokinase in the rat. Arch Biochem Biophys. 1968;127:17-21.
7. Furukawa Y. Enhancement of glucose-induced insulin secretion and modification of glucose metabolism by biotin. Nippon Rinsho. 1999;57:2261-2269.
8. Wang ZQ, Zhang XH, Cefalu WT. Chromium picolinate and biotin enhance glycogen synthesis and glycogen synthase gene expression in human skeletal muscle culture [abstract]. Diab Res Clin Pract. 2000;50:395.
9. Fernadez-Mejia C. Pharmacological effects of biotin. J Nutr Biochem. 2005;16:424-427.
10. Komorowski JR, Cefalu WT, et al. JCR-LA-cp rats showed improved lipid profiles in response to diets containing chromium picolinate and biotin. Appetite. 2001;36:230.
11. Albarracin C, Fuqua B, et al. Glycemic control is improved by the combination of chromium picolinate and biotin in type 2 diabetes mellitus [abstract]. Diabetes. 2004;53:A45(191-OR).
12. Singer GM, Geohas J. The effect of chromium picolinate and biotin supplementation on glycemic control in poorly controlled patients with type 2 diabetes mellitus: A placebo-controlled, double blinded, randomized trial. Diab Ther Tech. 2006;(8-6), in press.
13. Juturu V, Ruelle A, et al. Improved glycemic control after diabetes education and chromium picolinate/biotin supplementation in type 2 diabetes: Results from patients experience pilot program. Trace Elements Electrolytes. 2006;2:66-72.
14. Albarracin C, Fuqua B, et al. Effect of chromium picolinate and biotin combination on coronary risk lipids and lipoproteins in subjects with non HDL–C (>130 mg/dL) in type 2 diabetes mellitus [abstract]. Arterioscler Thromb Vasc Biol. 2005;25:E98-99 (abstr. P266).
15. Juturu V, Geohas J, et al. Chromium picolinate and biotin combination reduces coronary risk factors [abstract]. Arterioscler Thromb Vasc Biol. 2004;24:E66 (abstr. P88).
To comment on this article, contact
editor@uspharmacist.com.


