US Pharm. 2006;12:10-15.
Pharmacists who practiced in the 1970s may recall Povan, a red dye–derived medication once available for pinworm, and the seemingly endless number of prescriptions dispensed for it. This is in stark contrast to today's practice--prescriptions for anthelmintics to treat pinworm are rare. However, that does not necessarily mean that the prevalence of pinworm has decreased; since public awareness of this ancient parasite has dropped, it is less likely to be recognized when it is present.
Prevalence of Enterobiasis
Infestation with pinworm (
Enterobius vermicularis) is known as enterobiasis. This is the most
common helminth infestation in the United States, with an estimated 42 million
infested, translating to 14% of the population.1,2 Investigators in
other countries report much higher prevalences, such as 29% (Denmark), 39%
(Thailand), 50% (England), and 61% (India).1
Causative Agent
E. vermicularis is a white
nematode (roundworm) with a length of 8 to 13 mm for the adult female (about
the length of a standard staple) and 2 to 5 mm for the adult male.3
Its width is about 0.5 mm.1 The ova are oval objects appearing
microscopically to have three sides, approximately 55 x 25 mcm.1
Life Cycle/Transmission
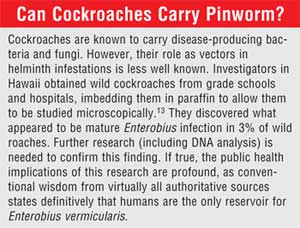
Humans are thought to be the sole
hosts of E. vermicularis (see sidebar).3,4 The common
residence of the adult pinworm is the large intestine, where it attaches to
the cecum and appendix.1 Following mating, the gravid female must
lay as many as 16,000 eggs.1 They live for an average of eight to
13 weeks.1,3 Although the reproductive habits of pinworm may be
unpleasant to contemplate, pinworms are equipped with the requisite instincts
to ensure survival of their species. The gravid mother will not lay eggs
inside the host, since the ability to spread throughout the population would
then be impaired. Rather, the female E. vermicularis has evolved the
strategy of exiting the anal opening to deposit the eggs in the folds of
perianal skin--a process known as ovipositing. Following
ovipositing, females reenter the anal opening. Successful reentry is termed
retroinfection.1
Freshly laid Enterobius eggs are not immediately capable of infestation, as the larvae must develop first. The eggs embryonate (develop the ability to infest a patient) within four to six hours. 1,3 If the environment is moist, they are potentially capable of infestation for 20 days. The newly laid eggs are surrounded by a sticky, albuminous material that allows them to adhere to the anal opening. To guarantee survival of the species, these eggs must reach another human's gastrointestinal tract, which can occur via several means.
An infested child might wear bed clothing that is sufficiently loose for the eggs to fall away as the host sleeps. If the eggs drop away at night, they could be found on sheets or blankets. The eggs are quite light and can be blown about by human activity, wind, or such activities as snapping egg-contaminated sheets while making the infested child's bed. Inhaled eggs may not enter the lungs, due to their weight and size, but may be deposited in the oropharynx, where they are easily swallowed.2
A second method of spread can occur during the day following ovipositing. The eggs can be easily removed from the anal skinfolds by scratching; the child then has viable eggs on his or her fingers or under the nails. As the child plays during the day, the eggs may be deposited on surfaces that other children's hands will have access to. Investigators visited homes and schools of infested children and identified pinworm eggs in 90% of samples taken from such diverse surfaces and locations as bars of soap, pet fur, swimming pools, walls of school dining rooms, and house dust samples. 5 If other children touching these surfaces subsequently place their fingers in their mouth to suck their thumb or bite their nails, the transmission loop is complete. Unfortunately, the child who originally had the infestation may also place his or her fingers inside the mouth, becoming reinfested and helping maintain a heavy parasite load--a process known as autoinfection.1
Clothing worn the next day might also be loose enough to allow the eggs to fall away and out of the clothing as the child plays and carries out routine activities. The eggs could deposit on carpets, floors, or playground equipment, or in a sandbox. Again, placing fingers in the mouth allows transmission to occur.
After the patient is infested, pinworms must hatch and mature before ovipositing begins. The average time from ingestion to detection of eggs in the perianal areas is four to six weeks.1
Epidemiology
Pinworm infestation is linked to
age, being most common in children of school age, followed by preschool
children.6,7 Adults are the least common age-group to experience
enterobiasis, with the exception of mothers whose children are infested.7
Children attending day care and other institutions are at greater risk for pinworm because of the high potential for transmission to those who are closely associated with the first case in the household. While some authors assert that pinworm crosses all social barriers, others state that poverty and poor personal hygiene increase the risk of infestation. 1,8,9
Manifestations
Symptoms may take weeks or even
months to become noticeable after the eggs are ingested.1 While one
third of those infested are asymptomatic, others begin to notice troubling
vague and nonspecific symptoms.1,10 The most common is anal,
perianal, and/or perineal pruritus, stimulated by movement of the female, and
albuminous substance that surrounds the eggs.1,8,9,11 Itching
worsens at night, when the female exits the anal opening.6 Other
manifestations are anorexia, abdominal pain, irritability, disturbed sleep,
insomnia, and restlessness.1,7
Ectopic Enterobiasis
Retroinfection via anal
reentrance does not occur via an organized search by the parasite; rather, the
parasite crawls blindly until a body orifice is detected. The search is not
always successful, and pinworms may enter other orifices, a process known as
ectopic enterobiasis. Ectopic enterobiasis is less common in males, as the
urinary opening is in a more distant location from the anal opening. However,
ectopic male infestation may cause urethritis or epididymitis. Female
physiology favors ectopic enterobiasis, as the vaginal and urethral openings
are in closer proximity to the anal opening. After pinworms have gained
entrance to the female genitourinary tract, they may cause vaginitis, vulvar
irritation, endometriosis, salpingitis, urethritis, pelvic inflammatory
disease, or pyelitis.1,12 The patient may notice such symptoms as
dysuria, enuresis, vaginal discharge, vulvovaginitis, or postmenopausal
bleeding.1
Prevention of Enterobiasis
Parents of patients infested with
pinworm may ask the pharmacist how to prevent a future problem and how to
maintain cleanliness during an ongoing episode. Several commonsense steps can
be followed to decrease the risk of reinfection. Most require added attention
to hygiene.6,7 For instance, the patient should shower every
morning to decrease the chance of spreading the parasite to others and of
retroinfection. Showering is preferable to bathing, since soaking in the bath
with eggs floating in the water could conceivably allow them to enter the
genitourinary tract. Patients should be urged to change underwear and
sleepwear each day and night. Each period of wear should be followed by
thorough washing. While the CDC advises against the practice, sheets could be
washed daily to remove eggs that fell onto them at night. If sheets are not
washed every day, they should be pulled back, and all blinds and curtains
should be opened during the day, as pinworm eggs are sensitive to sunlight.
Nails should be trimmed short. Children and adults must strive to keep their
fingers out of their mouths at all times. Hands must always be washed
thoroughly after bowel movements, especially during a bout of enterobiasis.
Hands should be washed before eating and after changing diapers. Children must
be urged to stop scratching their anal area, to prevent contaminating their
hands and to reduce their risk of excoriating the skin. Dressing them in
close-fitting underwear and cotton gloves can reduce or stop nocturnal
scratching. The floors should be vacuumed every other day, since eggs can
survive for two weeks on the carpet. Children may be allowed to return to day
care after the first treatment with pyrantel pamoate, if they have bathed and
nails are trimmed and cleansed.
Recognition/Treatment
The patient leaflet describes
steps to diagnose and treat enterobiasis. Patients may wish to provide a stool
sample; however, pinworms are seldom found in stool specimens, as they are not
usually released into the fecal stream.
The leaflet describes use of the only FDA-approved anthelmintic: pyrantel pamoate. The medication paralyzes the worm, causing it to lose its grip on the bowel lining and to be flushed from the body. Controversy surrounds the issue of FDA labeling versus recommendations from the CDC. The discrepancy stems from the fact that pyrantel pamoate is effective only for live worms and does not affect eggs or larvae. Thus, immature larvae and eggs that hatch after the first treatment remain fully viable and capable of beginning the infestation anew. The FDA-approved labeling states that the patient should take only one dose and take other doses only under the advice of a physician. However, the CDC states on a Web page devoted to patients: "With either prescription or over-the counter drugs.[sic] You should consult your health care provider before treating a suspected case of pinworm. Treatment involves a two-dose course. The second dose should be given 2 weeks after the first."7 This statement to patients effectively countermands and invalidates the FDA-approved labeling and gives tacit approval to the pharmacist to recommend a second dose.
Conclusion
Pinworm is a common but
seldom-recognized condition. An informed pharmacist can help infested patients
obtain appropriate treatment and prevent spread to other family members and
playmates.
References
1. Burkhart CN, Burkhart CG.
Assessment of frequency, transmission, and genitourinary complications of
enterobiasis (pinworms). Int J Dermatol. 2005;44:837-840.
2. Tsibouris P, Galeas T, Moussia M,
et al. Two cases of eosinophilic gastroenteritis and malabsorption due to
Enterobius vermicularis. Dig Dis Sci. 2005;50:2389-2392.
3. Enterobiasis. Centers for Disease
Control and Prevention. Available at:
www.dpd.cdc.gov/dpdx/HTML/Enterobiasis.htm. Accessed October 24, 2006.
4. Kucik CJ, Martin GL, Sortor BV.
Common intestinal parasites. Am Fam Physician. 2004;69:1161-1168.
5. Gale EA. A missing link in the
hygiene hypothesis? Diabetologia. 2002;45:588-594.
6. What you need to know about
threadworm. NursTimes. 2004;100:30.
7. Pinworm Infection. Centers for
Disease Control. Available at:
www.cdc.gov/NCIDOD/dpd/parasites/pinworm/factsht_pinworm.htm. Accessed October
24, 2006.
8. Otu-Bassey IB, Ejezie GC, Epoke J,
et al. Enterobiasis and its relationship with anal itching and enuresis among
school-age children in Calabar, Nigeria. Ann Trop Med Parasitol.
2005;99:611-616.
9. Singh SP, Panda C, Rout N, et al.
Anal albendazole application for pruritus ani in threadworm infestation. J
Trop Pediatr. 2005;51:386.
10. Petro M, Iavu K, Minocha A.
Unusual endoscopic and microscopic view of Enterobius vermicularis: a
case report with a review of the literature. South Med J.
2005;98:927-929.
11. Brown MD. Images in clinical
medicine: Enterobius vermicularis. N Engl J Med. 2006;354:e12.
12. Jain S, Sharma P, Gupta R. Dual
cervical parasitosis in a psychiatric patient. Cytopathology.
2005;16:53-54.
13. Chan OT, Lee EK, Hardman JM, et
al. The cockroach as a host for Trichinella and Enterobius
vermicularis: Implications for public health. Hawaii Med J.
2004;63:74-77.
To comment on this article, contact editor@uspharmacist.com.



