US
Pharm. 2006;6:72-77.
Whether preparing for a backyard
barbecue or an Amazon adventure, people need to take some simple steps to
avoid insect bites--practices that could protect them from potentially
life-threatening diseases carried by insects. The insects and other arthropods
that transmit disease to humans include mosquitoes, ticks, flies, chiggers,
fleas, and lice. From West Nile virus to malaria, these tiny vectors transmit
a host of diseases both here in the United States and abroad. Therefore, it is
important to be aware of the behavioral, physical, and chemical defenses
available.
Travel-Related Diseases
In 2004, approximately 763
million people worldwide traveled across international borders; most of them
were simply vacationing.1 Many travel destinations are developing
nations, where insect-borne diseases are more likely to occur. The Centers for
Disease Control and Prevention (CDC) receives reports of more than 1,000 cases
of malaria every year in people returning to the U.S. from other countries.
2 In fact, the most common cause of fever in someone returning from a
trip to the tropics is dengue fever--a viral disease in the family of yellow
fever--and malaria.3 However, travelling to Africa is not the
only way to encounter a potentially deadly mosquito-borne disease. West Nile
virus is transmitted by the Culex mosquito in all but a couple of
states in the U.S. In 2005, there were nearly 3,000 cases, with 116 deaths.
4 Although most people who use an insect repellent do so for mosquito
protection, they should also be aware of other arthropod-borne diseases such
as Lyme disease (tick bite), murine typhus (flea bite), and African sleeping
sickness (Tsetse fly bite). The CDC's Travelers' Health Web site
(www.cdc.gov/travel) can provide patients and health professionals with a vast
amount of information on diseases associated with travel. With a few
exceptions, if you don't get an insect bite, you can't get the disease it
carries.
Why People Get Bites
Mosquitoes are specially equipped
to find us during the day or night. They use a combination of visual,
chemical, and olfactory senses to locate a blood meal. From a distance,
mosquitoes that bite during the day can detect motion and bright colors.
Carbon dioxide, which we exhale and release from our skin, makes a powerful
attractant from up to 36 meters.5 Although we can't stop breathing,
people should avoid wearing strong perfumes and colognes or using scented
soaps, which may also attract mosquitoes. As the mosquito closes in, it can
still detect carbon dioxide, but it can also sense body heat and lactic acid,
all of which are increased with physical activity. Other factors that may
increase a person's chance of being bitten include being male, overweight, or
an adult.5 The type of mosquito and the availability of a primary
host other than people determine how aggressive a biter of humans they may be.
Many mosquitoes in South America, Africa, and Asia are aggressive biters--they
are less deterred by typical insect avoidance methods than our domestic ones
are. Thus, a higher level of insect precaution compliance is needed with
international travel.
PERSONAL PROTECTIVE MEASURES
Behavior Modification
If possible, people should avoid
typical insect habitats. These habitats may vary by geographic location, time
of the day, season, temperature, and urban versus rural environments. Heavily
forested areas or locations surrounding bodies of standing water, such as a
brackish lake, are more likely to be mosquito breeding grounds. Ticks prefer
low-lying brush in heavily wooded areas where they can sit and wait for a leg
to brush up against their perch. Since ticks do not jump or fly, they need
this close contact to attach to clothes where they can crawl to a bare part of
a leg and attach. Thus, visual inspection for attached ticks and then prompt
removal effectively minimizes the chance of acquiring a tick-borne infection.
The abundance of insects can be affected by
the temperature and season. Typically, mosquitoes are more common during
summer and fall months in temperate climates and following the rainy season in
the tropics. However, it takes only one bite by a mosquito carrying yellow
fever or malaria, for example, to transmit these deadly diseases. Thus, all
relevant insect precautions should be taken even when mosquito populations are
less intense.
Some mosquitoes are active at night and some
during the day. For example, peak biting times of the Aedes mosquito,
which carries yellow fever, dengue fever, and chikungunya viruses, are dawn
and dusk. The Anopheles mosquito carries malaria and bites only at
night between dusk and dawn. Knowing when certain mosquito-borne diseases are
more likely to be transmitted can help determine the appropriate intervention.
In some countries, such as Cambodia, both malaria and dengue fever occur,
necessitating the use of insect precautions day and night.
Insects may have a predisposition for rural
areas or for the city life. Dengue fever is an example of a disease spread by
an urban mosquito that has adapted its breeding grounds to places like old
tires, tin cans, or even puddles. Malaria, however, is mainly found in rural
areas of the tropics and subtropics, but there are notable exceptions, such as
India, where it occurs in rural and urban locations. When traveling to
malarious areas, it is important to know the cities to be visited, as some
have done a good job of mosquito breeding site cleanup, rendering the city
free of malaria. For example, in Nairobi, Kenya, there is no malaria, but
virtually everywhere else in Kenya it exists.
General advice for behavior modifications to
avoid insect bites would include staying indoors in a well-screened
air-conditioned room during peak biting times, avoiding outdoor exposure at
dusk, and not wearing bright clothing or perfumes.
Physical Barriers
Seek to put distance between you
and the blood-sucking insect looking for a meal. To protect against flying
insects, wear long-sleeved shirts and pants, as well as a hat. For ticks, make
sure to wear boots or other shoes that cover your ankles, and tuck your pants
into your shoes or socks. To decrease the chance of a mosquito biting through
your clothes, permethrin can be applied to clothing, or permethrin-treated
clothes can be purchased. Permethrin is a synthetic pyrethroid compound used
for its insecticide and insect repellent properties and is often referred to
as a "knock-down" insecticide. It is odorless, colorless, and won't affect the
material on which it is applied. This is the same chemical in products
available over the counter for killing head lice, so it is relatively safe. To
treat clothing before going out, apply a 0.5% spray to the surface of the
clothing, or soak clothing in a higher concentration. The treated clothes,
either sprayed or soaked, should protect for two weeks or two washings and up
to four weeks or six washings, respectively. When staying in regions where
insects bite at night, people should sleep under bed netting. In addition,
mosquito bed nets can be soaked in permethrin or purchased presoaked.
Insect Repellents
Whenever there is a risk of
contracting arthropod-borne disease, insect repellents should be applied to
exposed intact skin, never under clothing. Other general recommendations for
safe use of insect repellents are to apply it to an adult's hands and then to
the face with the hands, rather than spraying directly; never let young
children apply it to themselves; and wash off repellent when it is no longer
needed. Natural and synthetic repellents are available with variable efficacy
and safety.
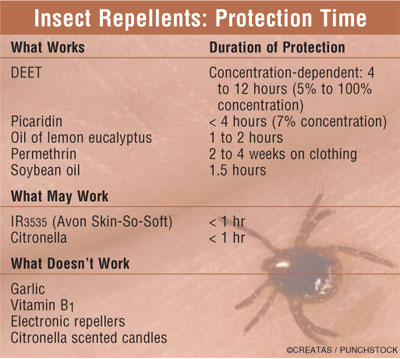
The CDC officially endorses two ingredients
with proven efficacy, DEET and picaridin, for domestic and international use.
For domestic mosquitoes, the CDC also sanctions the use of Environmental
Protection Agency (EPA)–registered repellents containing PMD (p-menthane
3,8-diol), the active ingredient of oil of lemon eucalyptus (for use in ages >=
3 years).6 See Table for a comparison of select repellents.
DEET:
The insecticide commonly known as DEET (now called N,N
-diethyl-3-methylbenzamide, formerly known as N,N-diethyl-meta-toluamide
) was developed for the military and was subsequently marketed to the public
in 1957. It is the most frequently used insect repellent in the world, with an
estimated 38% of the U.S. population applying it annually.7
Although the mechanism is not fully understood, it appears to interfere with
an insect's chemoreceptors for lactic acid. This broad-spectrum insect
repellent is relatively safe for adults and children and is the preferred
insect repellent, according to the CDC.8 DEET is an organic solvent
and in higher concentrations can dissolve synthetic material such as plastic
and rayon. The EPA considers it safe to humans and the environment. The
American Academy of Pediatrics considers it safe in concentrations between 10%
and 30%.9 DEET is available over the counter in concentrations
ranging from 5% to 100%. Above 50% concentration, little more protection is
gained, just increased duration of action. The optimal concentration for four
to six hours of protection is 20% to 35%. To increase the duration of action
to eight to 12 hours without having to increase the concentration beyond 20%
to 30%, sustained-release formulations are available.
When insect repellent is applied during the
day, people are often outside in the sun, where sunscreen is also necessary.
DEET repellents should be applied more than an hour after the application of
sunscreen, as DEET can reduce the effect of the sun protection factor (SPF) an
average of 33%.10 Combination DEET and sunscreen products should be
avoided, as they have not been clinically evaluated. It is estimated that for
every 10°C increase in outside temperature, 50% of an insect repellent's
duration of action is lost to evaporation.5 Thus, frequent
reapplication of DEET may be necessary, especially if one is swimming or
sweating excessively.
Picaridin:
Picaridin, also known as Bayrepel or KBR 3023, is a relatively new,
piperidine-based insect repellent in the U.S. It is touted as less irritating,
less smelly, and less damaging to clothing than DEET. Both DEET and picaridin,
however, are reported by the EPA to have a low potential for toxicity to
humans or the environment.11 Picaridin is marketed in the U.S. in a
concentration of 7%, but field testing with this compound was done on a 19.2%
concentration, roughly equivalent to DEET 20%.12 Thus, if you are
recommending picaridin, you should emphasize that it needs to be reapplied
more frequently than every four hours, especially in the tropics, due to the
low concentration available in the U.S.
Miscellaneous:
Although not originally introduced to repel insects, Avon's
Skin-So-Soft product was subsequently found to do so. The main ingredient is
butylacetylaminopropionate, or IR3535, an amino acid analog. IR3535 is
registered with the EPA as a pesticide against mosquitoes, ticks, and biting
flies, but it has a short duration of action. There is little clinical data on
IR3535, but in one large clinical study, it protected for only about 23
minutes.13
Botanicals:
Unlike the previous three synthetic insect repellents, the following are
derived from plant sources. Oil of lemon eucalyptus, also known as PMD, was
recently endorsed by the CDC against carriers of West Nile virus and other
domestic mosquitoes.6 This pleasant-smelling menthol-like repellent
at 30% is approximately equivalent to the protection of DEET 20% but does not
last as long; it must be applied more often than every four hours.
Citronella is a popular ingredient in
everything from sprays to candles and coils that are burned. Although it
smells nice, it offers less than an hour of protection per application; when
used as the candle or coil, it gives the same effect as does burning a regular
candle.7
The only other product clinically tested to
have protection against mosquitoes is a soybean oil–based product marketed as
Blocker. It provides protection similar to a 4.75% DEET or about 1.5 hours.
13
No other products have shown any clinically
proven efficacy, including vitamin B1 (thiamine) and garlic. In 1985, the
FDA responded to the increased anecdotal accounts of vitamin B1's
effectiveness as an insect repellent by issuing a statement refuting any
claims of efficacy and prohibiting manufacturers from doing the same for any
oral product.14
Treating the Bite
The main objective in caring for
mosquito bites is to reduce inflammation and itching that might lead to
superinfection of the bite site. Topical corticosteroids work fairly well at
reducing itching and inflammation. Oral antihistamines, particularly
cetirizine, also work well at reducing the redness and itching.15
An ammonium solution marketed as Afterbite was shown to be effective, at least
temporarily, in nearly everyone who used it.16
Conclusion
Although yellow fever and malaria
have been eradicated in the U.S. in the last century, other potentially deadly
mosquito-borne diseases such as West Nile virus and dengue fever have recently
emerged here. Thus, the need to protect against mosquitoes and other biting
arthropods both in the U.S. and abroad is great. Counseling patients on the
importance of personal protective measures will help to ensure safe and
enjoyable outdoor experiences.
References
1. Hill DR. The burden of illness
in international travelers. N Engl J Med 2006;354:115-117.
2. Shah S, Filler S, Causer LM, et
al. Malaria surveillance--United States, 2002. MMWR Surveill Summ
2004;53:21-34.
3. Freedman DO, Weld LH, Kozarsky PE,
et al. Spectrum of disease and relation to place of exposure among ill
returned travelers. N Engl J Med 2006; 354:119-130.
4. 2005 West Nile Virus Activity in
the United States. February 14, 2006. CDC Division of Vector-borne Infectious
Diseases. Available at: www.cdc.gov/ncidod/
dvbid/westnile/surv&controlCaseCount 06_detailed.htm. Accessed April 10, 2006.
5. Fradin MS. Insect protection. In:
Keystone J, Kozarsky P, Freedman D et al., eds. Travel Medicine. Mosby,
2004;61-69.
6. Updated Information Regarding
Mosquito Repellents. April 22, 2005. Centers for Disease Control and
Prevention. Available at:
www.cdc.gov/ncidod/dvbid/westnile/RepellentUpdates.htm. Accessed April 3, 2006.
7. Fradin, MS. Mosquitoes and
mosquito repellents: clinician's guide. Ann Intern Med
1998;128:931-940.
8. Centers for Disease Control and
Prevention. Protection against mosquitoes and other arthropods. In: Arguin PM,
Kozarsky PE, Navin AW, eds. Health Information for International Travel
2005-2006 (Yellow Book). Atlanta: US Department of Health and Human Services,
Public Health Service; 2005.
9. Flake ZA, Hinojosa JR, Brown M, et
al. Clinical inquiries. Is DEET safe for children? J Fam Pract
2005;54:468-469.
10. Montemarano AD, Gupta RK, Burge
JR, et al. Insect repellents and the efficacy of sunscreens. Lancet
1997;349:1670-1671.
11. Environmental Protection Agency:
New Pesticide Fact Sheet: Picaridin. 2005.
12. Frances SP, Waterson DGE, Beebe
NW et al. Field evaluation of repellent formulations containing DEET and
picaridin against mosquitoes in Northern Territory, Australia. J Med Entomol
2004;41:414-17.
13. Fradin MS, Day JF. Comparative
efficacy of insect repellents against mosquito bites. N Engl J Med
2002;347:13-18.
14. FDA. Drug products containing
active ingredients offered over-the-counter (OTC) for oral use as insect
repellents. Federal Register 1985;50,116 (21 CFR Part 310):25170-25171.
Available at
www.fda.gov/cder/otcmonographs/Insect_Repellent/insect_repellant_final_conclusions_19850617.pdf.
15. Reunala T, Brummer-Korvenkontio
H, Karppinen A, et al. Treatment of mosquito bites with cetirizine. Clin
Exp Allergy 1993;23:72-75.
16. Zhai H, Packman EW, Maibach HI.
Effectiveness of ammonium solution in relieving type I mosquito bite symptoms:
a double-blind, placebo-controlled study. Acta Derm Venereol
1998;78:297-298.
To comment on this article,
contact
editor@uspharmacist.com.



