US
Pharm. 2006;1:43-50.
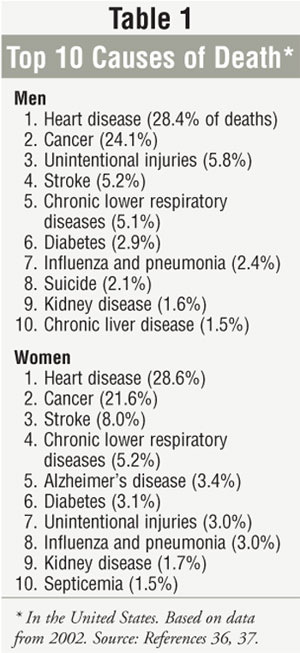
Chronic diseases including
cancer, diabetes, and cardiovascular disease are the leading causes of death
and disability in the United States (Table 1). Each year, chronic diseases
account for 70% of deaths and affect the quality of life of 90 million
Americans.1 While chronic diseases are the most common causes of
death in the U.S., many of them are preventable. Major risk factors include
lack of physical activity, smoking, and being overweight.2 Healthy
behaviors such as being physically active and avoiding tobacco use can reduce
the risk of death from chronic disease and can prevent or control their
devastating effects.1 Other major causes of morbidity and mortality
in the U.S., such as unintentional injury and stroke, can also be reduced
through patient education.3-5
Common Health Risks
Coronary
artery disease (CAD):
CAD is the most common type of heart disease and the leading cause of death in
both men and women in the U.S., resulting in more than 500,000
deaths each year.6 The disease occurs when the coronary arteries
become hardened and narrowed as a result of plaque buildup on artery walls.
6 Uncontrollable risk factors for CAD include age (e.g., risk increases
after age 45 for men and after age 55 for women), family history of heart
disease, having a father or brother diagnosed with the disease at age 55 or
younger, and having a mother or sister diagnosed at age 65 or younger.6
Controllable risk factors include high blood cholesterol, high blood pressure
(BP), smoking, diabetes, lack of physical activity, and being overweight.
6
It is recommended that
patients who have had a myocardial infarction, unstable angina, ischemic
stroke, or transient ischemic attacks use prophylactic aspirin therapy if not
contraindicated.7 In patients at high risk for a future cardiac
event, the benefits of aspirin therapy should be weighed against the risk for
potential complications. In low-risk patients, possible hemorrhagic
complications may outweigh the benefits; current data do not support the use
of prophylactic aspirin therapy in this population.8
Cancer:
Cancer is the second-leading cause of death in men and women, while lung
cancer is the leading cause of cancer-related death in the U.S.9
Risk factors for cancer vary; cancers of the lung, mouth, larynx, bladder,
kidney, cervix, esophagus, and pancreas are related to tobacco use, while skin
cancer is related to unprotected exposure to strong sunlight.4
Risk factors for cancer
include age and family history. Gender can also increase the risk of certain
cancers (e.g., women are more likely than men to develop breast cancer), while
the risk of some cancers (e.g., prostate cancer) increases with age.4
About 75% of all cancers in the U.S. are caused by environmental
factors (e.g., tobacco use, poor diet, infectious disease, exposure to
chemicals and radiation) and about one third of all cancer-related deaths
result from dietary factors and lack of physical activity in adulthood.4
Unintentional injuries:
Accidents are a leading cause of death for Americans of all ages, regardless
of gender, race, or economic status.3 In 2003, more than 27 million
people experienced a nonfatal unintentional injury that required a visit to an
emergency department.3
In 2003, motor vehicle
accidents (42,900), poisoning (14,500), and falls (14,200) were the leading
causes of accident-related deaths in the U.S.10 To reduce injuries,
the National Safety Council recommends learning first aid and cardiopulmonary
resuscitation and encourages installing handrails, grab bars, and night-lights
in homes to prevent falls, and storing all medications and cleaners in
childproof cabinets to reduce poisonings.10
Stroke:
Stroke, a disease that occurs when blood flow to the brain is interrupted, is
the leading cause of serious long-term disability and the third-leading cause
of death in the U.S.11 Every 45 seconds, an American has a stroke.
12 Treatable risk factors include high BP, smoking, heart disease, and a
history of stroke and diabetes.13 Warning signs include sudden
numbness or weakness of the face, arm, or leg (especially on one side of the
body), confusion or trouble speaking or understanding, trouble seeing in one
or both eyes, trouble walking, dizziness, loss of balance or coordination, and
severe headache with no known cause.14
Chronic obstructive
pulmonary disease (COPD):
COPD, a group of chronic lung conditions that includes emphysema and chronic
bronchitis, is the fourth-leading cause of death in the U.S. and is projected
to be the third-leading cause of death by 2020.15 While about 24
million adults in the U.S. have impaired lung function, only 12.1 million
adults over age 25 reported diagnosis of COPD in 2001, indicating that the
disease is underdiagnosed.16
Smoking tobacco is the most
common cause of COPD.15 Other risk factors include chronic exposure
to air pollution, chemical fumes, and certain dusts.15 While most
patients with lung cancer will develop COPD (since both diseases are caused
primarily by smoking), only 1% to 2% of patients with COPD will develop lung
cancer.17
Diabetes:
Diabetes, a chronic metabolic disorder characterized by abnormalities in
carbohydrate, fat, and protein metabolism, is a leading cause of blindness,
kidney disease, neuropathy, amputation, skin disorders, gastroparesis, and
depression.18 While about two out of three people with diabetes in
the U.S. die from heart attack or stroke, the disease is underreported as a
cause of death; studies have found that only 35% to 40% of patients with
diabetes had the disease mentioned on their death certificate and the disease
was listed as the underlying cause of death in only 10% to 15% of patients.
19,20
Risk of type 2 diabetes
increases with age and degree of obesity and is more prevalent in Native
American, Hispanic, and African American populations. Other risk factors
include past gestational diabetes or giving birth to a baby 9 pounds or
heavier, high BP, an abnormal serum lipid profile, a sedentary lifestyle
(exercising fewer than three times per week), and having a parent or sibling
with the disease.21
Influenza and pneumonia:
Each year, influenza affects 5% to 20% of Americans and results in more than
200,000 hospitalizations and about 36,000 deaths.5 Symptoms of flu
include fever, chills, fatigue, cough, headache, and muscle aches.22
Streptococcal pneumonia is the most common cause of community-acquired
pneumonia, accounting for 25% to 35% of all cases and an estimated 40,000
deaths each year.23
Pneumonia, a general term for
infection and inflammation of the lungs, is caused mainly by infections from
viruses, bacteria, and mycoplasmas; other causes include fungal infections or
inhalation of liquid, gases, or dust.23 Children, the elderly, and
people with underlying health problems (e.g., COPD, diabetes) are at high risk
for pneumonia. Pneumonia and influenza are preventable by vaccination.
Kidney disease:
In 2002, kidney disease was the ninth-leading cause of death in the U.S.,
accounting for 40,974 deaths.24 Overuse of over-the-counter
analgesics such as acetaminophen, aspirin, and NSAIDs and macrolide
antibiotics can damage the kidneys; an estimated 3% to 5% of all new cases of
chronic kidney failure may be caused by chronic overuse of these medications.
25
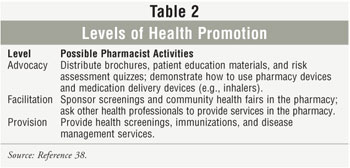
The Role of the Pharmacist
Screening and
educating patients on reducing risk factors can help prevent or reduce their
risk of developing chronic disease.26-28 Pharmacists should assess
a patient's current health status and disease risk factors, including weight,
BP, vaccination history, family history of chronic disease, and information
regarding lifestyle (e.g., smoking, physical activity).29 Possible
pharmacist activities are listed in Table 2.
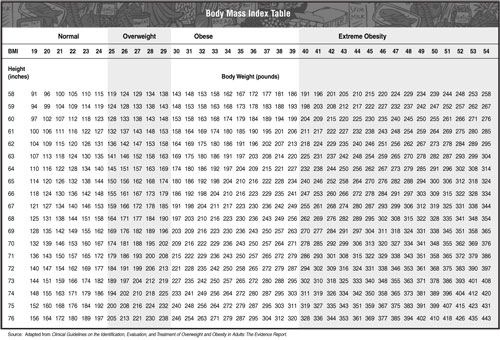
Weight loss:
Pharmacists should provide patients who are overweight with information on
beginning a weight loss program and advise them to achieve a body weight as
close to ideal for their height as possible. Identifying an individual who is
overweight involves measuring body mass index (BMI), waist circumference, and
risk factors for diseases and conditions associated with obesity. Waist
circumference (measurement of the largest point of the abdomen) is associated
with an increased risk of heart disease if greater than 40 inches in men
and 35 inches in women. BMI, a measure of body fat based on an individual's
height and weight, can determine whether an individual is underweight (less
than 18.5), normal weight (18.5 to 24.9), overweight (25 to 29.9), or obese
(30 or greater). Losing 5% to 15% of body weight can significantly improve
health (BMI Chart).30
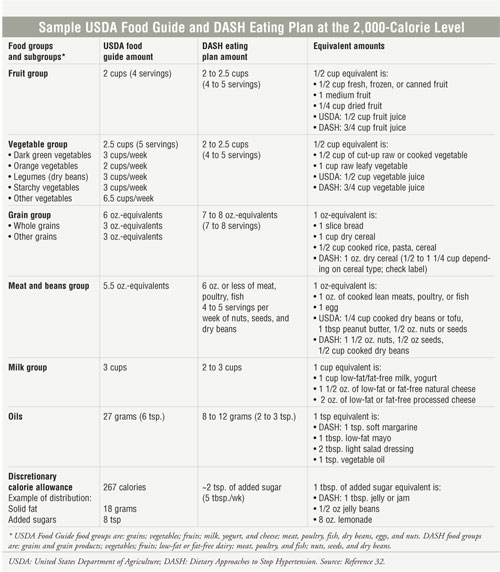
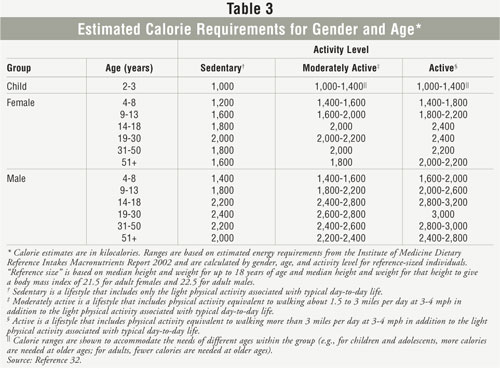
Diet:
Consuming nutrient-dense foods, limiting the intake of saturated and trans
fats, cholesterol, sugar, salt, and alcohol, and meeting recommended calorie
requirements can help reduce the risk of chronic disease (Table 3). A balanced
eating plan such as the U.S. Department of Agriculture (USDA) Food Guide or
the Dietary Approaches to Stop Hypertension (DASH) can help patients achieve
their calorie requirements. A sample USDA Food Guide and DASH Eating Plan at
the 2,000 calorie level can be found below.
Goals of any weight management plan
should be safe and intended to improve the patient's health status and
minimize future health-related problems.29 Regularly checking a
patient's weight and waist measurements can help ensure compliance with the
plan.29 Regular BP readings may also encourage compliance, since
most people with elevated BP on the DASH diet experience a decrease in BP,
sometimes in as little as two weeks.31
Exercise:
Physical activity is crucial to good health and can have health benefits,
including a decreased risk of coronary heart disease.2 To reduce
the risk of chronic disease in adulthood, individuals should engage in 30
minutes of moderately intense physical activity most days of the week in
addition to regular daily activities. To manage weight, 60 minutes of moderate
to vigorous physical activity and not exceeding calorie requirements is
recommended. Weight loss requires 60 to 90 minutes of moderately intense
physical activity and not exceeding calorie requirements.32
A well-rounded exercise plan
includes aerobic, muscle strengthening, and stretching activities. Patients
should begin an exercise regimen slowly with small goals, such as walking 10
minutes a day three days per week. Patients are more likely to exercise if
they like an activity and should be encouraged to select one they enjoy.33
Smoking cessation:
Smoking cessation has major and immediate health benefits for men and women of
all ages. People who quit smoking before age 50 have half the risk of dying in
the next 15 years as compared with those who continue to smoke.27
Pharmacists can conduct screening programs and provide specialized services
that focus on such areas as hypertension, diabetes, asthma, patient education,
or general medication management.28 Pharmacists have proved to be
effective smoking cessation counselors that can improve success rates.34
A smoking cessation program is available on the Washington State Pharmacy
Association Web site at www.wsparx.org/sitemap.asp.
Vaccination:
Pharmacists can help improve vaccination rates to reduce the risk of death
from influenza and pneumococcal pneumonia.35 Influenza vaccination
should be considered in children six to 23 months of age, people 65 years or
older, residents of long-term care facilities, individuals six months to 18
years old on long-term aspirin therapy (due to the risk of Reye's syndrome),
women who are pregnant during the flu season, people with nerve or muscle
disorders (e.g., seizure disorders, cerebral palsy) and weakened immune
systems, and anyone in close contact with these high-risk populations.
Conclusion
While lack of
physical activity, smoking, and being overweight are major risk factors for
the leading causes of morbidity and mortality in American adults, pharmacists
are ideally trained and positioned to help reduce these risk factors. Patients
should be given achievable, measurable goals and specific information
regarding calorie intake, activity levels, vaccines, and use of smoking
cessation products to maximize results. Pharmacists who choose to become
involved in improving the health of patients can make a difference.
REFERENCES
1. Centers for Disease Control.
Chronic Disease Prevention. Available at: http://www.cdc.gov/nccdphp.
2. Centers for Disease
Control and Prevention and National Institutes of Health. Healthy People 2010.
Heart Disease and Stroke. Available at:
www.cdc.gov/cvh/hp2010/objectives.htm#ref15.
3. Centers for Disease
Control. Unintentional Injury Prevention Program Activity Report 2004.
Available at: www.cdc.gov/ncipc/pub-res/unintentional_
activity/2004/index2004.htm.
4. American Cancer
Society. Cancer Reference Information. What Are the Risk Factors for Cancer?
Available at:
www.cancer.org/docroot/CRI/content/CRI_2_4_2x_What_are_the_risk_factors_for_
cancer_72.asp?sitearea=.
5. Centers for Disease
Control and Prevention. Influenza Fact Sheet. Available at: www.cdc.gov/
flu/keyfacts.htm.
6. National Heart,
Lung, and Blood Institute. Diseases and Conditions Index: Coronary Heart
Disease. Available at: www.nhlbi.nih.gov/health/dci/
Diseases/Cad/CAD_WhatIs.html.
7. American Heart
Association. Aspirin in Heart Attack and Stroke Prevention. Available at:
www.americanheart.org/presenter. jhtml?
identifier=4456.
8. Awtry EH, Loscalzo
J. Aspirin. Circulation. 2000;101:1206-1218.
9. National Cancer
Institute. NIH Senior Health. Lung Cancer. Available at:
http://nihseniorhealth. gov/lungcancer/lungcancerdefined/01.html.
10. National Safety
Council. Report on Injuries in America. Available at: www.nsc.org/library/
report_injury_usa.htm.
11. Centers for Disease
Control and Prevention. Morbidity and Mortality Weekly Report. Public Health
and Aging: Atrial Fibrillation as a Contributing Cause of Death and Medicare
Hospitalization. Available at: www.cdc.gov/mmwr/preview/
mmwrhtml/mm5207a2.htm.
12. American Stroke
Association. Heart Disease and Stroke Statistics 2005 Update. Available at:
www.americanheart.org/presenter.jhtml?
identifier=3000090.
13. National Institute
of Neurological Disorders and Stroke. Brain Basics: Preventing Stroke.
Available at: www.ninds.nihgov/disorders/stroke/
preventing_stroke.htm.
14. American Stroke
Association. Stroke Warning Signs. Available at: www.strokeassociation.org/
presenter.jhtml?identifier=4742.
15. National Heart,
Lung and Blood Institute. Diseases and Conditions Index: Chronic Obstructive
Pulmonary Disease. Available at: www.nhlbi.nih.gov/health/dci/Diseases/Copd/
Copd_WhatIs.html.
16. National Heart,
Lung and Blood Institute. Chronic Obstructive Pulmonary Disease Data Fact
Sheet. NIH Publication No. 03-5229. March 2003.
17. Dr. Per Grinsted.
Lung Cancer. Available at: www.netdoctor. co.uk/diseases/facts/lungcancer.htm.
18. American Diabetes
Association. Type 2 Diabetes Complications. Available at: www.diabetes.org/
type-2-diabetes/complications.jsp.
19. American Diabetes
Association. Make the Link! Diabetes, Heart Disease, and Stroke. Available at:
www.diabetes.org/type-2-diabetes/well-being/heart-disease-and-stroke.jsp.
20. National Diabetes
Clearinghouse. National Diabetes Statistics. Deaths Among People With Diabetes
2002. Available at: http://diabetes. niddk.nih. gov/dm/pubs/statistics/#12.
21. National Diabetes
Clearinghouse. Am I at Risk for Type 2 Diabetes? NIH Publication No. 04-4805.
April 2004. Available at: http://diabetes. niddk.nih.gov/dm/pubs/riskfortype2/.
22. Department of
Health and Human Services. Centers for Disease Control and Prevention.
National Immunization Program. Vaccine Information Statement: Inactivated
Influenza Vaccine. October 20, 2005.
23. American Lung
Association. Pneumonia Fact Sheet. Available at: www.lungusa.org/site/pp.asp?
c=dvLUK9O0E&b=35692.
24. Centers for Disease
Control. National Center for Health Statistics. Kidney Disease. Available at:
www.cdc.gov/nchs/fastats/kidbladd.htm.
25. National Kidney
Foundation. Kidney Disease. Analgesics. Available at: www.kidney.org/atoz/
atozItem.cfm?id=23.
26. Centers for Disease
Control and Prevention and National Institutes of Health. Healthy People 2010.
What Are Its Goals? Available at: www.healthypeople.gov/about/goals.htm.
27. Centers for Disease
Control and Prevention and National Institutes of Health. Healthy People 2010.
Objectives for Improving Health. Available at: www.healthypeople.gov/Document/
tableofcontents.htm#Volume2.
28. Babb VJ, Babb J.
Pharmacist involvement in Healthy People 2010. J Am Pharm Assoc. 2003;
43:56-60.
29. Rovers JP, Currie
JD, Hagel HP, et al. A practical guide to pharmaceutical care. American
Pharmaceutical Association; 1998.
30. National Institute
of Diabetes & Digestive & Kidney Diseases. Better Health and You. Available
at: http://win.niddk.nih.gov/publications/better_health.htm#healthyweight.
31. The DASH Eating
Plan. NIH Publication No. 03-4082. 1998; Revised May 2003.
32. Department of
Health and Human Services and Department of Agriculture. Dietary Guidelines
for Americans 2005. Chapter 4: Physical Activity. Available at:
www.health.gov/dietaryguidelines/dga2005/ document/html/chapter4.htm.
33. National Heart,
Lung, and Blood Institute. The Dash Eating Plan. Available at:
www.nhlbi.nih.gov/ health/public/heart/hbp/dash.
34. Zillich AJ, Ryan M,
Adams A, et al. Effectiveness of a pharmacist-based smoking-cessation program
and its impact on quality of life.
Pharmacotherapy
. 2002;22:759-765.
35. Grabenstein JD,
Guess HA, Hartzema AG, et al. Effect of vaccination by community pharmacists
among adult prescription recipients. Med Care. 2001;39:340-348.
36. Centers for Disease
Control and Prevention. Leading Causes of Death--Males, 2002. Available at:
www.cdc.gov/men/lcod.htm#all.
37. Centers for Disease
Control and Prevention. Leading Causes of Death--Females, 2002. Available at:
www.cdc.gov/od/spotlight/nwhw/lcod.htm#all.
38. Ciardulli LM, Goode
JV. Using health observances to promote wellness in community pharmacies. J
Am Pharm Assoc. 2003;43:63.
To comment on this article,
contact
editor@uspharmacist.com.



