US Pharm.
2008;33(3):HS10-HS15.
Over the past two decades,
pain assessment and management in children has greatly improved due in part to
the development of age-specific pain assessment tools and a better
understanding of the role of analgesics in this population. In the
postoperative setting, different surgical procedures will produce varied
levels of pain, and sound practices that account for the alterations in
pharmacokinetics and pharmacodynamics that are present in children should be
incorporated into the management of such pain. Many children still suffer from
unnecessary pain due to misconceptions regarding pain control.1
These misconceptions include the belief that children do not perceive pain the
same way as adults, and some clinicians may believe that analgesics are
associated with an increased incidence of toxicity in this population.2
A thorough understanding of the assessment techniques and therapeutic
interventions utilized for postoperative analgesia will allow the pharmacist
to play an integral role in the management of the pediatric patient.
Assessment
Pain assessment tools utilized in
the postoperative setting should be appropriate to reflect the needs of each
child and should account for any limitations that may hinder accurate
assessment. For example, children less than 4 years of age may be considered
too young to properly utilize a self-report pain scale.3 A commonly
used assessment tool is the Wong-Baker FACES Rating Scale, where children are
asked to look at and choose from six different faces that depict expressions
associated with no pain to varying levels of pain that may or may not be
associated with crying. This tool is effective in children as young as 3 years
old; however, its one-dimensional nature limits its usefulness in evaluating
the behavioral effects that may accompany a painful experience.
With regard to the
postoperative setting, one study recommended the use of two scales for pain
assessment in the pediatric patient.3 These included the Face,
Legs, Arms, Cry, Consolability (FLACC) scale for hospitalized patients and the
Parents' Postoperative Pain Measure (PPPM) for discharged patients.4,5
The FLACC scale provides a quantitative measure of the presence and severity
of pain in children via assessment of pain-related behaviors.4 The
PPPM scale is a 15-item checklist that allows parents to assess their child's
pain.5 The COMFORT scale, comprised of six behavioral items and two
physiologic items, has also been validated for use in the postoperative
setting in children 0 to 3 years of age.6
Pharmacotherapy
Nonopioid
Analgesics: Nonopioid
analgesics, including nonsteroidal anti-inflammatory drugs (NSAIDs) and
acetaminophen, play an important role as first-line agents in the management
of mild-to-moderate pain in children.7-12 Depending on the level of
pain control required, these agents may be sufficient as the sole
pharmacologic treatment or may be used adjunctively with opioids or other
types of pain control. NSAIDs, in particular, have proven to be a popular
method for analgesia in the postoperative setting. Their ease of dosing,
widespread availability, parental acceptance, lack of opioid-type adverse
effects, and the relative comfort of the practitioner in prescribing such
drugs support their role in postoperative pain management. When used in
combination with opioids, NSAIDs exhibit "opioid-sparing" effects.
8 Consequently, the patient is likely to experience fewer adverse
effects associated with both analgesics.
Common adverse effects of
NSAIDs include bleeding and gastrointestinal and nephrotoxic effects. However,
one placebo-controlled study of ketorolac in postoperative infants showed no
adverse effects on renal or hepatic function.9 NSAIDs are
contraindicated in a number of pediatric patients, including those who are
susceptible to renal or hepatic disorders, have increased bleeding risks, or
are on other nephrotoxic agents or anticoagulants; use should also be avoided
in neonates.10
Cyclooxygenase-2 (COX-2)
inhibitors are starting to be evaluated in the pediatric patient.11
However, their place in therapy remains to be fully elucidated. The current
lack of studies and underwhelming evidence gives minimal support to the use of
COX-2 inhibitors over NSAIDs for children.10,12
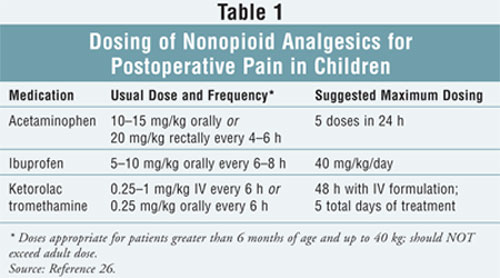
Acetaminophen, an inhibitor of
prostaglandin synthesis, is commonly used in the treatment of mild
postoperative pain; however, compared to other agents, its analgesic potency
remains low and ceiling effects may be observed.8 Acetaminophen is
frequently used with codeine to enhance the overall analgesic effect. Loading
and maintenance dosing regimens vary with age; newborns metabolize
acetaminophen via sulfation pathways, while in adults metabolism occurs mainly
via glucuronidation pathways in the liver. This difference leads to a slightly
extended plasma half-life in the neonate.13 Consideration for use
should always be given to patients with potential contraindications (e.g.,
viral hepatitis, decreased glutathione stores). Recommended dosing for
nonopioid analgesics in children can be found in TABLE 1.
Opioid Analgesics:
With proper dosing and appropriate assessment and monitoring, opioid
analgesics can be considered for the treatment of moderate-to-severe
postoperative pain. The underutilization of opioids in the pediatric
population may arise from the misconception that pain perception is diminished
secondary to immature pain-processing pathways. However, anatomical components
that facilitate pain perception are well-formed at 25 weeks' gestation,
although the ability to mount descending analgesic responses develops later
during infancy.14,15Opioid receptors also develop during gestation
and are considered to be widely distributed.14,15 The neurobiology
of pain in infants and children dictates that opioids can provide effective
analgesia. Nonetheless, it is imperative that clinicians understand the
pharmacokinetic and pharmacodynamic factors associated with the use of opioid
analgesics in the pediatric population before these agents are considered.
The response to an opioid
analgesic varies greatly by age. In neonates, opioids are more likely to
induce respiratory distress secondary to poor ventilatory reflexes.15
With regard to drug metabolism, newborns may be at an increased risk of
opioid accumulation due to immature hepatic enzymes. Additionally, the renal
excretion of opioids may be diminished secondary to decreased glomerular
filtration rate and renal tubular secretion capacity.15 Newborns
and infants have a greater percentage of total body water, thereby producing
an alteration in the volume of distribution of these agents. The half-life of
morphine is markedly increased in neonates compared to adults (six to eight
hours versus two hours, respectively).16 By adolescence, the
metabolism and excretion of opioids reach the same levels seen in adults.
Morphine has been extensively
studied for the management of pain after major surgery in children.17,18
It is considered a favorable choice because it is well tolerated and can be
given through several different routes of administration, although oral
administration is typically avoided because of variable bioavailability.19
Other opioids that have been utilized in this setting include fentanyl,
hydromorphone, codeine, and tramadol.12,19,20 Fentanyl and
hydromorphone are suitable alternatives to morphine secondary to their ease of
titration when given parenterally. Because codeine and tramadol have the
ability to produce weaker analgesic effects, use is typically limited to the
management of moderate to moderately severe pain associated with minor
procedures.19 Additionally, tramadol has been associated
with increased postoperative nausea and vomiting, further restricting its use.
20
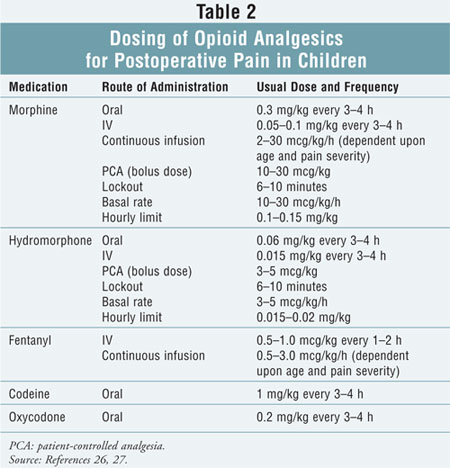
The recommended dosing for
opioid analgesics for the management of postoperative pain in children can be
found in TABLE 2. These agents should be administered around the clock,
rather than as needed, to avoid "chasing" increases in pain severity. As
previously mentioned, children are at an increased risk for the development of
opioid-induced respiratory depression and are not invulnerable to other
adverse effects (e.g., pruritus, sedation); therefore, adherence to dosing and
titration guidelines is essential. Monitoring of adverse effects should occur
along with, and as frequently as, the assessment of the child's pain.
The use of opioid infusions
(e.g., patient-controlled analgesia [PCA], continuous IV infusions) has become
commonplace in the management of pediatric postoperative pain. Continuous IV
infusions provide consistent analgesia and are frequently used in neonates,
infants, and select children with severe pain who have undergone major surgery
or have been admitted to intensive care units.21 PCA has been shown
to be an effective means of pain control in older children (above 5 to 7 years
of age) and adolescents who can understand the use of such a device. PCA
provides the patient with analgesia by maintaining steady serum opioid
concentrations and allows for patient-specific dose adjustments. Morphine is
considered the opioid of choice for PCA and continuous IV infusions, with
hydromorphone reserved for those who cannot tolerate, or do not achieve
analgesia with, morphine.
Adjuvant Analgesics
Local anesthetics,
including bupivacaine and ropivacaine, have frequently been used in children
for analgesia during and immediately following surgery; however, it is
important to be aware of their associated risks. It can be particularly
difficult to detect intravascular infiltration in children, and cardiovascular
toxicity and seizures have been reported in this population.20 When
added to a single injection of a local anesthetic epidural solution, clonidine
1 to 2 mcg/kg has enhanced the duration and effectiveness of the local
anesthetic.22
As an N
-methyl-D-aspartate (NMDA) receptor antagonist, dextromethorphan is another
adjuvant analgesic agent that has shown mixed results in postoperative pain
control. One study demonstrated that a one-time preoperative dose of 0.5 to 1
mg/kg of oral dextromethorphan did not reduce postoperative morphine
consumption in children.23 A potential benefit to using
dextromethorphan is its lack of unwanted opioid adverse effects. Ketamine,
also an NMDA receptor antagonist, may be beneficial in epidural administration
due to the lack of observed respiratory depression.20 One
meta-analysis identified a median dose of 0.4 mg/kg of ketamine used among all
trials examined, with some evidence to support the use of ketamine in children.
24 However, limitations to using this agent as adjunctive therapy may
include the relative difficulty of obtaining preservative-free products for
epidural use and the potential of ketamine to induce emergence phenomena,
nausea, and vomiting.
Summary
Inappropriate management of
postoperative pain in children can result in changes that could have a lasting
negative impact. Goals of therapy should include providing complete pain
relief while minimizing adverse physiologic and psychological effects.
Pharmacists can play a crucial role in implementation, initiation, and
monitoring of appropriate analgesic therapies25 and should
participate in age-appropriate preprocedural teaching and postoperative
counseling. Pharmacists can also partake in research that focuses on the
integration of "adult" medicine into the pediatric population and can be key
decision-makers in the development and implementation of staff education,
standardized order sets and protocols, and thorough follow-up procedures.
Future directions for
pediatric postoperative pain management include the need for further studies
on adjuvant nonopioid pain control as well as continued validation of
pediatric postoperative pain measurement scales.
REFERENCES
1. Forgeron PA, Finley GA, Arnaout M. Pediatric pain prevalence and parents' attitudes at a cancer hospital in Jordan. J Pain Symptom Manage. 2006;31:440-448.
2. Rieman MT, Gordon M. Pain management competency evidenced by a survey of pediatric nurses' knowledge and attitudes. Pediatr Nurs.2007;33:307-312.
3. von Baeyer CL, Spagrud LJ. Systematic review of observational (behavioral) measures of pain for children and adolescents aged 3 to 18 years. Pain. 2007;127:140-150.
4. Merkel SI, Voepel-Lewis T, Shayevitz JR, Malviya S. The FLACC: a behavioral scale for scoring postoperative pain in young children. Pediatr Nurs. 1997;23:293-297.
5. Chambers CT, Reid GJ, McGrath PJ, Finley GA. Development and preliminary validation of a postoperative pain measure for parents. Pain. 1996;68:307-313.
6. van Dijk M, de Boer JB, Koot HM, et al. The reliability and validity of the COMFORT scale as a postoperative pain instrument in 0- to 3-year-old infants. Pain. 2000;84:367-377.
7. Sutters KA, Miaskowski C, Holdridge-Zeuner D, et al. A randomized clinical trial of the effectiveness of a scheduled oral analgesic dosing regimen for the management of postoperative pain in children following tonsillectomy. Pain. 2004;110:49-55.
8. Morton NS. Management of postoperative pain in children. Arch Dis Child Educ Pract Ed. 2007;92:ep14-ep19.
9. Lynn AM, Bradford H, Kantor ED, et al. Postoperative ketorolac tromethamine use in infants ages 6ñ18 months: the effect on morphine usage, safety assessment, and stereo-specific pharmacokinetics. Anesth Analg. 2007;104:1040-1051.
10. Hil·rio MO, Terreri MT, Len CA. Nonsteroidal anti-inflammatory drugs: cyclooxygenase 2 inhibitors. J Pediatr (Rio J). 2006;82(suppl 5):S206-S212.
11. Stempak D, Gammon J, Klein J, et al. Single-dose and steady-state pharmacokinetics of celecoxib in children. Clin Pharmacol Ther. 2002;72:490-497.
12. Young D. FDA advisers endorse Celebrex for juvenile rheumatoid arthritis: lack of studies in children raises safety concerns. Am J Health Syst Pharm. 2007;64:11-12.
13. Van Lingen RA, Deinum JT, Quak JM. Pharmacokinetics and metabolism of rectally administered paracetamol in preterm neonates. Arch Dis Child Fetal Neonatal Ed. 1999;80:F59-F63.
14. Lonnqvist PA, Morton NS. Postoperative analgesia in infants and children. Br J Anaesth. 2005;95:59-68.
15. Goldschneider KR, Mancuso TJ, Berde CB. Pain and its management in children. In: Loeser JD, ed. Bonica's Management of Pain. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2001.
16. Kart T, Christrup L, Rasmussen M. Recommended use of morphine in neonates, infants and children based on a literature review: part 1ñpharmacokinetics. Paediatric Anaesth. 1997;7:5-11.
17. Lynn AM, Nespeca MK, Bratton SL, Shen DD. Intravenous morphine in postoperative infants: intermittent bolus dosing versus targeted continuous infusions. Pain. 2000;88:89-95.
18. Lynn AM, Nespeca MK, Opheim KE, Slattery JT. Respiratory effects of intravenous morphine infusions in neonates, infants, and children after cardiac surgery. Anesth Analg. 1993;77:695-701.
19. Kokinksy E, Thornberg E. Postoperative pain control in children: a guide to drug choice. Pediatr Drugs. 2003;5:751-762.
20. Verghese ST, Hannallah RS. Postoperative pain management in children. Anesth Clin N Am. 2005;23:163-184.
21. Kost-Byerly S. New concepts in acute and extended postoperative pain management in children. Anesth Clin N Am. 2002;20:115-135.
22. Eisenach JC, De Kock M, Klimscha W. Alpha(2)-adrenergic agonists for regional anesthesia. A clinical review of clonidine (1984-1995). Anesthesiology. 1996;85:655-674.
23. Rose JB, Cuy R, Cohen DE, Schreiner MS. Preoperative oral dextromethorphan does not reduce pain or analgesic consumption in children after adenotonsillectomy. Anesth Analg. 1999;88:749-753.
24. Elia N, TramËr MR. Ketamine and postoperative pain--a quantitative systematic review of randomised trials. Pain. 2005;113:61-70.
25. Ingelmo PM, Gelsumino C, Acosta AP, et al. Epidural analgesia in children: planning, organizing and development of a new program. Minerva Anestesiol. 2007;73:575-585.
26. Taketomo CK, Hodding JH, Kraus DM, eds. Lexi-Comp's Pediatric Dosage Handbook. 12th ed. Hudson, OH: Lexi-Comp; 2005.
27. Denman WT, Ballantyne J.
Postoperative pain in children. In: Ballantyne J, Fishman SM, Abdi S, eds.
The Massachusetts General Hospital Handbook of Pain Management. 2nd ed.
Philadelphia, PA: Lippincott Williams & Wilkins; 2002:306-321.
To comment on this article, contact
editor@uspharmacist.com.


