US Pharm.
2008;33(11):Epub.
Attention-deficit/hyperactivity
disorder (ADHD) and learning disability (LD) are two of the most prevalent
disorders occurring in children aged 6 to 17 years. In 2006, the National
Centers for Health Statistics (NCHS) estimated that 4.5 million and 4.6
million children, respectively, have been diagnosed with ADHD or LD.
Prescriptions for ADHD medications have increased dramatically in the past
decade, with utilization in many states more than quadrupling, but the reason
for the increase is not clear. The reason for the recent decline in the use of
drugs that contain methylphenidate also is not known. The annual societal cost
of illness for ADHD has been estimated to be between $36 and $52 billion (in
2005 dollars). Studies have demonstrated increases in substance abuse,
risk-taking, and criminal behaviors among adolescents who have ADHD and other
related disorders.
According to the NCHS, nearly
5% of children had ADHD without LD, 5% of children had LD without ADHD, and 4%
of children had both disorders. The percentage of children aged 6 to 17 years
who had ADHD increased at an annual rate of 3% from 1997 through 2006, but the
percentage of children with LD did not change significantly. No significant
change was found in the percentage of children aged 6 to 11 years who had
ADHD; however, an annual increase of 4% occurred among those aged 12 to 17
years.
An increase in the percentage
of children with ADHD occurred among both boys (2%) and girls (4%). The causes
and risk factors contributing to ADHD are unknown, although the disorder
appears to be more prevalent among boys.
Children whose birthweight was
low (14.1%) were more likely than children who did not have a low birthweight
(8.1%) to have LD. Among low-birthweight children, 7.5% and 7.9% of boys were
more likely to have ADHD and LD, respectively, in comparison with girls (3%
and 7.4%, respectively).
Hispanic children (5.3%) were
less likely than non-Hispanic black children (8.6%) and non-Hispanic white
children (9.8%) to have ADHD. No significant racial or ethnic differences were
found in the percentage of children having LD without ADHD.
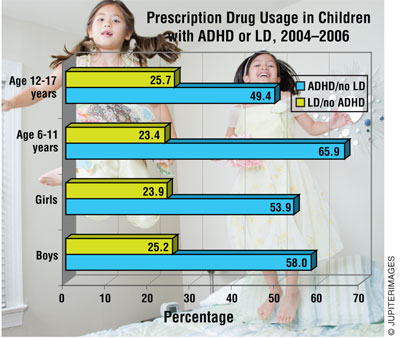
Children with ADHD (46.2%)
were more likely than children without ADHD (4%) to have contact with a
mental-health professional, utilize more prescription medications (62.7% vs.
10.6%), and make frequent health care visits (56.7% vs. 21.7%). Children with
LD were more likely (59.3%) than children without this disorder (2.4%) to
utilize special-education services.
The prevalence of mental
retardation (6.5%), hearing or vision problems (4.5%), and allergies (36.8%)
was lowest among children who had ADHD without LD; children who had LD without
ADHD had the highest prevalence of mental retardation (36.6%). Children who
had both ADHD and LD had the highest prevalence of hearing or vision problems
(9.6%) and allergies (42.8%). The prevalence of asthma was lowest (20.8%)
among children having LD without ADHD, and it was highest (22.2%) among
children who had both.
Children with Medicaid
coverage (5.9%) were more likely than uninsured (2.6%) and privately insured
children (3.1%) to have ADHD, LD, or both disorders. These children also were
more likely to utilize health care and special-education services.
To comment on this article,
contact rdavidson@jobson.com.



