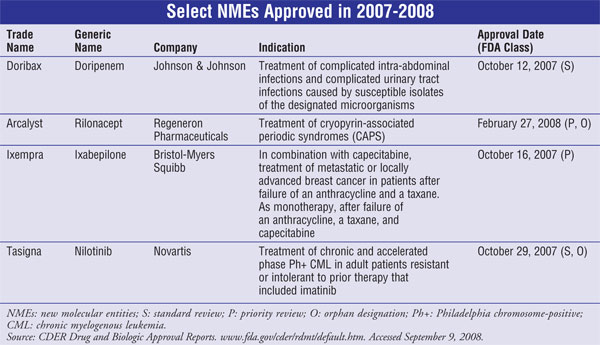
US Pharm. 2008;33(10):HS5-HS17.
New molecular entities
(NMEs), as defined by the FDA, are new drug products containing, as their
active ingredient, a chemical substance marketed for the first time in the
United States. The following descriptions of NMEs approved in 2007-2008 (TABLE)
include a brief summary of the clinical and pharmacologic profile for each new
drug, as well as selected pharmacokinetics, adverse reactions, drug
interactions, and dosing information. This review is intended to be objective
rather than evaluative in content. The information for each NME was obtained
primarily from sources published prior to FDA approval. Experience has shown
that many aspects of a new drug's therapeutic profile, such as adverse
reactions, do not emerge until after the drug is used in large numbers of
patients for several years. Hence, while this review offers a starting point
for learning about new drugs, it is essential that practitioners become aware
of changes in a drug's therapeutic profile over time.
Doripenem (Doribax, Johnson
& Johnson)
Indication
and Clinical Profile1-3:
Doripenem is a new carbapenem beta-lactam antibacterial approved for treatment
of complicated intra-abdominal infections (cIAIs) and complicated urinary
tract infections (cUTIs), including pyelonephritis. Approximately two million
intra-abdominal procedures are performed in the U.S. annually, and cIAIs are a
common cause of hospitalization following these surgeries. Urinary tract
infections (UTIs) account for at least 40% of all hospital infections.
Although many cases of UTI are uncomplicated, a significant proportion are
classified as "complicated" because of anatomical abnormalities in the urinary
tract, which make clearance of bacteria more difficult or cause kidney
infection (pyelonephritis). Both cIAIs and cUTIs can be caused by a broad
range of bacteria, many of which are resistant to multiple antibiotics.
The efficacy of doripenem for
the treatment of cIAIs was evaluated in two identical controlled studies
involving 946 adult patients who were treated with 500 mg of doripenem or with
1 g of meropenem administered IV every eight hours. After at least three days
of therapy, patients were permitted to switch to oral amoxicillin 875
mg/clavulanate 125 mg twice daily, for a total of five to 14 days of IV and
oral treatment. Doripenem was shown to be as effective as meropenem in
clinical cure rates 25 to 45 days posttreatment.
The efficacy of doripenem for
the treatment of cUTIs was evaluated in two multicenter studies involving
1,171 adult patients. In the first study, patients were treated with either
500 mg of doripenem IV (over 1 hour q8h) or with 250 mg levofloxacin IV every
24 hours. The second study was noncomparative but was otherwise of similar
design. In both studies, patients were permitted to switch to oral
levofloxacin (250 mg every 24 hours) after at least three days of IV therapy,
for a total of 10 days of IV and oral treatment. Doripenem was as effective as
levofloxacin with regard to the microbiological eradication rates 5 to 11 days
posttreatment.
Pharmacology and
Pharmacokinetics1-3:
Doripenem is a synthetic, parenteral carbapenem antibiotic. Like all other
members of the beta-lactam class, this drug acylates and inactivates essential
bacterial penicillin-binding proteins resulting in inhibition of cell wall
biosynthesis and bacterial cell death. Like other carbapenems, doripenem is
effective against a wide range of gram-positive and gram-negative pathogens
often implicated in cIAI and cUTI including Escherichia coli, Bacteroides
fragilis, viridans group streptococci, Proteus species, Klebsiella
pneumoniae, and Pseudomonas aeruginosa. P. aeruginosa, a
gram-negative bacterium with increasing multidrug resistance, is one of the
leading causes of hospital-acquired (nosocomial) infections. In general, there
are relatively few antibiotics available or in development to treat these
life-threatening gram-negative infections.
The pharmacokinetics of
doripenem (Cmax and AUC) are linear over the therapeutic dose
range, and there is no evidence of drug accumulation following multiple IV
infusions in patients with normal renal function. Plasma protein binding is
low (8%), and the median volume of distribution is 16.8 L, similar to
extracellular fluid volume (18.2 L). Doripenem penetrates into several bodily
fluids and tissues, including those at the site of infection.
Doripenem is not a substrate
for hepatic CYP450 enzymes. A small amount of metabolism to an inactive
ring-opened metabolite occurs primarily via renal dehydropeptidase-I.
Doripenem is primarily eliminated unchanged by the kidneys by both glomerular
filtration and tubular secretion. The mean plasma terminal elimination
half-life of doripenem is approximately one hour. At therapeutic doses, 70%
and 15% of the dose is excreted in the urine as unchanged drug and the
ring-opened metabolite, respectively, within 48 hours. Less than 1% of the
total dose is eliminated in the feces.
No dosage adjustment of
doripenem appears necessary based on gender, race, or age or in patients with
normal renal function. However, based on the clearance profile, dosage
adjustment is necessary in patients with moderate (CrCl 31-50 mL/min) and
severe (CrCl
<30 mL/min) renal impairment. Presently, there is
insufficient information to make dosage adjustment recommendations in patients
on hemodialysis or with hepatic impairment.
Adverse Reactions1-3:
The most common adverse reactions (>=5%) observed in clinical trials with
doripenem included headache, nausea, diarrhea, rash, and phlebitis. Serious,
potentially fatal hypersensitivity reactions have been reported occasionally
in patients treated with beta-lactam antibiotics. Therefore, before doripenem
therapy is instituted, it should be determined if a patient has had a previous
hypersensitivity reaction to other beta-lactam drugs (e.g., carbapenems,
cephalosporins, penicillins) or other allergens. Nearly all antibacterial
agents have been reported to cause Clostridium difficile–associated
diarrhea (CDAD), ranging from mild diarrhea to fatal colitis. If CDAD is
suspected or confirmed, antibiotic use should be discontinued and appropriate
treatment measures implemented. Doripenem is a Pregnancy Category B drug and
should be used with caution while nursing. The safety and effectiveness in
pediatric patients have not been established.
Drug Interactions1-3:
Significant reductions in serum valproic acid concentrations have been
reported in patients receiving carbapenem antibiotics, resulting in concerns
about loss of seizure control. It appears that carbapenem antibiotics may
inhibit valproic acid glucuronide hydrolysis, and thereby enhance its
elimination. Thus, serum valproic acid concentrations should be monitored
frequently after initiating therapy with any carbapenem, or alternative
antibacterial or anticonvulsant therapy be considered. Probenecid, an
inhibitor of active tubular secretion, causes an increase in plasma
concentrations of doripenem, and thus concurrent use is not recommended.
Dosage and Administration1-3:
To reduce the development of drug-resistant bacteria and maintain
effectiveness, doripenem (and all antibacterials) should be used only to treat
infections that are proven or strongly suspected to be caused by susceptible
bacteria, preferably documented by culture and susceptibility data. Doripenem
is supplied in single-use, clear glass vials containing 500 mg of sterile
doripenem powder. The recommended dosage for indicated infections is 500 mg
administered every eight hours by IV infusion over one hour, in patients 18
years of age or older. The duration of therapy for intra-abdominal infections
is five to 14 days, and 10 days for cUTIs. For patients with significant renal
impairment, dosage reduction is recommended. Patients with an estimated CrCl >=30
to
<50 mL/min should receive 250 mg every eight hours, while those
with a CrCl between 10 and 30 mL/min should receive 250 mg every 12 hours.
Full details for preparations of IV solutions are provided in the
manufacturer's literature.
Rilonacept (Arcalyst,
Regeneron Pharmaceuticals)
Indication
and Clinical Profile4,5:
Rilonacept is approved for the long-term treatment of two cryopyrin-associated
periodic syndromes (CAPS) in patients aged 12 years or older. Specifically, it
is approved for the familial cold auto-inflammatory syndrome (FCAS) and
Muckle-Wells syndrome (MWS) forms of the disease. CAPS are inherited disorders
caused by mutations in the nucleotide-binding domain, leucine rich family,
pyrin domain containing 3 (NLRP-3) gene, which encodes the protein cryopyrin.
Cryopyrin regulates the protease caspase-1 and controls activation of
interleukin-1 beta (IL-1ß). Mutations in NLRP-3 can cause an overactive
inflammasome, resulting in excessive levels of activated IL-1ß, which causes
inflammation, joint pain, rash or skin lesions, fever and chills, eye redness
or pain, and fatigue. The FCAS and MWS disorders are extremely rare, affecting
about 300 people in the U.S. MWS is associated with more severe inflammation
and amyloidosis and may include hearing loss or deafness.
The approval of rilonacept was
based on results from a two-part trial designated as Part A and Part B. In
Part A, patients received a 320-mg loading dose of rilonacept followed by 160
mg/wk or placebo for six weeks. In Part B, all patients received rilonacept
160 mg/wk for nine weeks and were then randomized to either rilonacept 160
mg/wk or placebo for an additional nine weeks. The trial also included a
24-week, open-label treatment extension phase; enrolled patients received
rilonacept 160 mg/wk. For both parts of the study, patients completed a daily
questionnaire to rate the severity (0-10, none to very severe) of the primary
symptoms of CAPS. In Part A, the mean symptom score reductions from baseline
to end point among rilonacept recipients was 2.4 versus a 0.5 among placebo
recipients. The mean symptom change among rilonacept patients in Part B of the
trial was 0.1 versus a 0.9 difference among placebo-treated patients. Most
patients indicated improvement in symptom scores within several days of
initiating rilonacept therapy. Rilonacept therapy was associated with a
20-mg/L reduction from baseline in mean C-reactive protein (CRP) levels versus
a 2-mg/L reduction with placebo, and mean serum amyloid A (SAA) levels were
reduced by 56 mg/L versus no change among placebo-treated patients. Reductions
in mean symptom scores, serum CRP, and SAA levels were maintained for one year
or less among patients who received rilonacept in the extension phase of these
trials.
Pharmacology and
Pharmacokinetics4,5:
Rilonacept acts as a soluble decoy receptor that binds the excessive IL-1‚
formed in CAPS, thereby preventing its interaction with cell surface receptors
and significantly reducing the inflammation associated with disease.
Rilonacept also binds IL-1a and IL-1 receptor antagonist (IL-1ra) with reduced
affinity. The equilibrium dissociation constants for rilonacept binding to
IL-1ß, IL-1a, and IL-1ra are reported to be 0.5 pM, 1.4 pM, and 6.1 pM,
respectively.
Rilonacept is administered
subcutaneously (SC), and steady state is reached by six weeks. Gender, age,
and body weight (50-120 kg) do not appear to have a significant effect on
trough levels. The effect of race could not be assessed because only Caucasian
patients participated in the clinical study (reflecting disease epidemiology).
No pharmacokinetic data are available in patients with hepatic or renal
impairment.
Adverse Reactions4,5:
The most commonly reported side effects associated with use of rilonacept
include injection-site reactions, upper respiratory infections, cough, and
hypoesthesia. Infections appear to result from the IL-1 blocking actions of
the drug that interfere with immune response. Some patients receiving
rilonacept experienced serious, life-threatening infections. Thus, patients
with active or chronic infections should not be treated with rilonacept, and
patients should receive all recommended vaccinations before initiating
treatment with this drug. Rilonacept is a Pregnancy Category C drug. Live
vaccines should not be administered concurrently with rilonacept.
Drug Interactions4,5:
Specific drug interaction studies have not been conducted with rilonacept.
However, concurrent administration of drugs that block IL-1 with a
TNF-blocking agent (e.g., etanercept, infliximab, adalimumab) has been
associated with an increased risk of serious infections and an increased risk
of neutropenia; thus, it is not recommended. In addition, the concomitant
administration of rilonacept and other agents that block IL-1 or its receptors
(IL-1ra) is not recommended.
Increased levels of cytokines,
including interleukins during chronic inflammation, can suppress the formation
of CYP450 enzymes. Thus, it is expected that exposure to drugs that bind to
IL-1, such as rilonacept, could result in normalization of CYP450 enzyme
levels. This may be clinically relevant for CYP450 substrates with a narrow
therapeutic index, where the dose is individually adjusted (e.g., warfarin)
and may require monitoring and dosage adjustment.
Dosage and Administration4,5:
The first injection of rilonacept should be performed under the supervision of
a qualified health care professional. If patients or caregivers are to
administer rilonacept, they should be instructed on aseptic reconstitution and
methods of administration. Rilonacept is supplied in single-use, 20-mL glass
vials containing 220 mg of the drug as a lyophilized powder. The recommended
dosage for patients aged 18 years or older is a 320-mg loading dose (delivered
as two 2-mL SC injections of 160 mg on the same day, administered in different
injection sites), followed by 160 mg/wk administered as a single 2-mL SC
injection. The recommended dosage of rilonacept for patients aged 12 to 17
years is a 4.4-mg/kg loading dose (maximum 320 mg), delivered as one or two SC
injections (maximum single-injection volume 2 mL). Pediatric patients should
be treated with 2.2 mg/kg/wk delivered as a single SC injection (maximum 2 mL).
Ixabepilone (Ixempra,
Bristol-Myers Squibb)
Indication
and Clinical Profile6-8:
Ixabepilone was approved for use in combination with another cancer drug,
capecitabine, for the treatment of patients with metastatic or locally
advanced breast cancer resistant to treatment with an anthracycline
(doxorubicin or epirubicin) and a taxane (paclitaxel or docetaxel), or whose
cancer is taxane resistant and for whom further anthracycline therapy is
contraindicated. The drug is also approved as monotherapy for the treatment of
metastatic or locally advanced breast cancer in patients whose tumors are
resistant or refractory to anthracyclines, taxanes, and capecitabine. About
180,000 new cases of breast cancer are diagnosed in the U.S. each year.
Metastatic breast cancer is the most advanced stage of breast cancer and has
the potential to spread to almost any region of the body.
The efficacy of ixabepilone in
combination with capecitabine was assessed in a multicenter trial in which
patients were assigned either to IV ixabepilone (40 mg/m2 every 3
weeks) plus capecitabine (1,000 mg/m2 twice daily for 2 weeks)
followed by one week of rest or to capecitabine (1,250 mg/m2 twice
daily) for two weeks followed by one week of rest. Eligible patients (n = 752)
had been treated previously with anthracyclines and taxanes and had
demonstrated tumor progression or resistance to these agents. Patients in the
combination therapy group received a median of five treatment cycles. The
combination treatment prolonged progression-free survival compared to
capecitabine alone (5.7 months vs. 4.1 months), with a statistically
significant 25% decrease in the risk of disease progression. An objective
response rate was observed in more than twice as many subjects in the
combination group compared to control (34.7% vs. 14.3%). The median duration
of response was 6.4 months versus 5.6 months.
The efficacy of ixabepilone as
monotherapy was assessed in a single-arm trial in which ixabepilone was
administered at a dosage of 40 mg/m2 over three hours every three
weeks. Eligible patients (n = 126) had tumors that had recurred or progressed
after two or more chemotherapy regimens including an anthracycline, a taxane,
and capecitabine. Patients received a median of four treatment cycles.
Independent radiologic review demonstrated clinically significant tumor
shrinkage in 12% of the ixabepilone-treated patients, with a median duration
of response of 6.0 months.
Pharmacology and
Pharmacokinetics6-8:
Ixabepilone is a semisynthetic analog of epothilone B. It binds directly to
ß-tubulin subunits on microtubules, resulting in suppression of the dynamic
instability of aß-II and aß-II microtubules. This arrests the cells in
the G2-M phase of the cell cycle and induces tumor cell apoptosis. In addition
to direct antitumor activity, ixabepilone also has antiangiogenic activity.
Ixabepilone is active in xenografts that are resistant to multiple agents
including taxanes, anthracyclines, and vinca alkaloids and has demonstrated
synergistic antitumor activity in combination with capecitabine in vivo.
The pharmacokinetics of
ixabepilone appear to be linear at therapeutic doses. The mean volume of
distribution of 40 mg/m2 ixabepilone at steady state is in excess
of 1,000 L, and plasma protein binding ranges from 67% to 77%. Ixabepilone is
extensively metabolized by hepatic CYP3A4 oxidation. More than 30 inactive
metabolites are excreted into urine and feces, and no single metabolite
accounts for more than 6% of the administered dose. Approximately 86% of the
dose is eliminated within seven days in feces (65% of the dose) and in urine
(21% of the dose), primarily as metabolites. Ixabepilone has a terminal
elimination half-life of approximately 52 hours. The pharmacokinetics of
ixabepilone are not significantly altered by gender, race, or age.
Adverse Reactions6-8:
The most common adverse events associated with ixabepilone treatment include
peripheral sensory neuropathy, fatigue/asthenia, nausea, myalgia/arthralgia,
alopecia, diarrhea, palmar-plantar erythrodysesthesia syndrome, vomiting,
stomatitis/mucositis, anorexia, musculoskeletal pain, constipation, abdominal
pain, nail disorder, and myelosuppression (primarily manifested as
neutropenia). In clinical trials, patients with hepatic impairment at baseline
experienced greater toxicity with ixabepilone treatment, including occurrences
of febrile neutropenia and severe adverse reactions. Thus, the drug carries a
black box warning concerning toxicity in patients with moderate or severe
hepatic impairment. A greater incidence of cardiac adverse reactions,
including myocardial ischemia and ventricular dysfunction, was observed among
ixabepilone-treated patients than among patients treated with capecitabine
alone in clinical trials. Ixabepilone should not be taken by patients who have
had severe allergic reactions to drugs that contain cremophor or its
derivatives (e.g., polyoxyethylated castor oil). Ixabepilone should avoided in
pregnancy and nursing (Pregnancy Category D).
Drug Interactions6-8:
Ixabepilone is a CYP3A4 substrate and thus has the potential to interact with
other drugs that are inducers or inhibitors of this cytochrome isozyme.
Ixabepilone does not inhibit CYP enzymes at therapeutic concentrations and is
not expected to alter the plasma concentrations of other drugs.
Coadministration of ixabepilone with potent CYP3A4 inhibitors (e.g.,
ketoconazole) can result in a significant increase in ixabepilone AUC. If
alternative treatment cannot be administered, a dosage adjustment should be
considered. The effect of mild or moderate inhibitors (e.g., erythromycin,
fluconazole, verapamil) on exposure to ixabepilone has not been studied.
Therefore, caution should be exercised when administering mild or moderate
CYP3A4 inhibitors during treatment with ixabepilone.
Strong CYP3A4 inducers (e.g.,
dexa methasone, phenytoin, carbamazepine, rifampin, rifampicin, rifabutin,
phenobarbital) may decrease ixabepilone concentrations, leading to
subtherapeutic levels. St. John's wort may decrease ixabepilone plasma
concentrations unpredictably and should be avoided. While capecitabine and
ixabepilone may alter each other's AUC and Cmax values, this
interaction is not clinically significant.
Dosage and Administration6-8:
Ixabepilone is supplied as a single-use kit containing one vial of ixabepilone
powder and one vial of diluent to be reconstituted for IV administration. All
patients should be pretreated with a histamine H1and H2 antagonist
approximately one hour before ixabepilone infusion to reduce the risk of
hypersensitivity reactions. The recommended initial dosage is 40 mg/m2
administered IV over three hours every three weeks. Doses for patients with
body surface area exceeding 2.2 m2 should be calculated based on
2.2 m2. If toxicities occur, delay treatment and allow for
recovery. If toxicities recur upon reinitiation, an additional dosage
reduction of 20% is recommended. Patients with hepatic impairment receiving
ixabepilone monotherapy require dose reductions based on aspartate
aminotransferase (AST), alanine aminotransferase (ALT), and bilirubin levels.
Dosage adjustment should be followed according to product labeling.
Nilotinib (Tasigna,
Novartis)
Indication
and Clinical Profile9-11:
Nilotinib is indicated for the treatment of chronic phase and accelerated
phase Philadelphia chromosome–positive (Ph+) chronic myelogenous leukemia
(CML) in adult patients resistant or intolerant to prior therapy that included
imatinib. CML accounts for 15% of all leukemias in adults, and approximately
4,500 new cases of CML were diagnosed in 2007. An abnormal chromosome (Ph) is
present in leukemic cells of the majority of CML patients. Imatinib is used
for the treatment of newly diagnosed patients with Ph+ CML.
FDA approval of nilotinib was
based on the results of a multicenter trial involving patients with
imatinib-resistant or -intolerant CML with separate cohorts for chronic phase
(CML-CP) and accelerated phase (CML-AP) disease. Overall, 280 CML-CP subjects
with a minimum follow-up of six months and 105 CML-AP subjects with a minimum
follow-up of four months were enrolled. A major cytogenetic response was
observed in 40% of the subjects. Complete response was observed in 28%, and
partial response was observed in 12% of this group. The efficacy end point in
the CML-AP arm confirmed hematologic response, defined as either a complete
hematologic response or no evidence of leukemia. A confirmed hematologic
response was observed in 26%, with 18% showing a complete hematologic response
and 8% showing no evidence of leukemia. Median duration of response had not
been reached at the time of approval for either group. However, based on
current data, 59% of the CML-CP subjects with a major cytogenetic response and
63% of CML-AP subjects with a confirmed hematologic response each had a
duration of response of at least six months.
Pharmacology and
Pharmacokinetics9-11:
Nilotinib is a signal transduction inhibitor of the BCR-ABL kinase, c-KIT, and
platelet-derived growth factor (PDGF), all of which play a role in cell
proliferation, cell migration, and angiogenesis. Nilotinib binds to and
stabilizes the inactive conformation of the kinase domain of the ABL protein.
In vitro, nilotinib inhibits BCR-ABL–mediated proliferation of murine leukemic
cell lines and human cell lines derived from Ph+ CML patients. In vivo,
nilotinib was shown to reduce tumor size in a murine BCR-ABL xenograft model.
Nilotinib is administered
orally, and bioavailability increases significantly when given with a high-fat
meal. Peak concentrations are reached three hours after oral administration.
Serum protein binding is high (98%) and the blood-to-serum ratio of nilotinib
is 0.68. Inter-patient variability in nilotinib AUC was 32% to 64%. The
elimination half-life is estimated to be approximately 17 hours. The primary
pathways of nilotinib metabolism include oxidation and hydroxylation, but the
parent drug is the main circulating component in the serum. None of the
metabolites appear to contribute significantly to the pharmacologic activity.
More than 90% of the administered dose is eliminated within seven days, mainly
in feces (93%). Parent drug accounted for 69% of the dose. The
pharmacokinetics of nilotinib are not significantly altered by age, body
weight, gender, or ethnic origin.
Adverse Reactions9-11:
In clinical trials, the most commonly reported adverse reactions (>10%)
associated with nilotinib therapy were rash, pruritus, nausea, fatigue,
headache, constipation, diarrhea, and vomiting. Less common, but more severe,
adverse effects included thrombocytopenia, neutropenia, pneumonia, febrile
neutropenia, leukopenia, intracranial hemorrhage, elevated lipase, and
pyrexia. Nilotinib has been reported to cause concentration-dependent QT
prolongation, prompting a black box warning for possible life-threatening
irregular heartbeat and sudden death. Patients should consult with their
physician about avoiding other medications that can cause heart problems when
taking nilotinib. Women are advised to avoid breastfeeding or becoming
pregnant while taking nilotinib (Pregnancy Category D).
Drug Interactions9-11:
Nilotinib is metabolized by CYP3A4, and concurrent administration of strong
inhibitors (e.g., ketoconazole) or inducers (e.g., rifampicin) of this
cytochrome isozyme have the potential to increase or decrease systemic
exposure (i.e., AUC) to nilotinib. Nilotinib is also a competitive inhibitor
of CYP3A4, CYP2C8, CYP2C9, CYP2D6, and UGT1A1 and therefore has the potential
to increase the concentrations of drugs metabolized by these enzymes. Thus,
caution should be exercised when coadministering nilotinib with drugs that are
substrates for these CYP isozymes, and substrates such as warfarin that have a
narrow therapeutic index should be avoided, if possible. Nilotinib may induce
CYP2B6, CYP2C8, and CYP2C9, and thus has the potential to decrease the
concentrations of drugs that are cleared by these isozymes. Nilotinib is a
substrate for and inhibitor of human P-glycoprotein transporters, so caution
should be exercised when it is used with other drugs that are substrates or
inhibitors of this transporter.
Dosage and Administration9-11:
Nilotinib is supplied as 200-mg hard gelatin capsules in blister packs. The
recommended initial dosage is 400 mg orally twice daily, at 12-hour intervals.
No food should be consumed at least two hours before and one hour after
administration of nilotinib. Treatment should continue as long as the patient
does not show evidence of progression or unacceptable toxicity. Nilotinib may
be given in combination with hematopoietic growth factors (e.g., eryth
ropoietin), hydroxyurea, or anagrelide if clinically indicated. Dosage
adjustments or modifications should be followed according to the product label
for patients with ECGs with a QTc greater than 480 msec; for those with
neutropenia and/or thrombocytopenia; for those with Grade 3 or greater
elevations of serum lipase, amylase, bilirubin, or hepatic transaminases; and
for patients with other clinically significant moderate or severe
nonhematologic toxicities. The concomitant use of strong CYP3A4 inhibitors and
strong CYP3A4 inducers with nilotinib should be avoided, if possible, or else
dosage adjustment is required.
REFERENCES
1. Doribax
(doripenem for injection) package insert. Raritan, NJ: Ortho-McNeil
Pharmaceutical, Inc; October 2007.
2. Fritsche TR,
Stilwell MG, Jones RN. Antimicrobial activity of doripenem (S-4661): a global
surveillance report (2003). Clin Microbiol Infect. 2005;11:974-984.
3. Bhavnani SM, Hammel
JP, Cirincione BB, et al. Use of pharmacokinetic-pharmacodynamic target
attainment analyses to support phase 2 and 3 dosing strategies for doripenem. Antimicrob
Agents Chemother. 2005;49:3944-3947.
4. Arcalyst
(rilonacept) package insert. Tarrytown, NY: Regeneron Pharmaceuticals, Inc;
February 2008.
5. FDA approves new
orphan drug for treatment of rare inflammatory syndromes. February 27, 2008.
www.fda.gov/bbs/topics/news/2008/new01801.html. Accessed February 28, 2008.
6. Ixempra Kit (ixabepilone
for injection) package insert. Princeton, NJ: Bristol-Myers Squibb Company;
October 2007.
7. Thomas E, Tabernero
J, Fornier M, et al. Phase II clinical trial of ixabepilone (BMS-247550), an
epothilone B analog, in patients with taxane-resistant metastatic breast
cancer. J Clin Oncol. 2007;25:3399-3406.
8. Denduluri N, Low JA,
Lee JJ, et al. Phase II trial of ixabepilone, an epothilone B analog, in
patients with metastatic breast cancer previously untreated with taxanes. J
Clin Oncol. 2007;25:3421-3427.
9. Tasigna (nilotinib)
package insert. East Hanover, NJ: Novartis; October 2007.
10. Breccia M, Cannella
L, Nanni M, et al. Nilotinib can override dasatinib resistance in chronic
myeloid leukemia patients with secondary resistance to imatinib first-line
therapy. Acta Haematol. 2007;118:162-164.
11. Kantarjian HM,
Giles F, Gattermann N, et al. Nilotinib (formerly AMN107), a highly selective
BCR-ABL tyrosine kinase inhibitor, is effective in patients with Philadelphia
chromosome-positive chronic myelogenous leukemia in chronic phase following
imatinib resistance and intolerance. Blood. 2007;110:3540-3546.
To comment on this article, contact
rdavidson@jobson.com.



